

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
In recent years, the widespread use of screening mammography and breast ultrasonography (US) has resulted in the increased detection of nonpalpable breast lesions that require percutaneous biopsy [1,2]. Surgical resection is needed if lesions are diagnosed as malignant or high-risk, or show a discordance between imaging and pathologic findings.
A simple and stable localization method is essential for the removal of these lesions, and many methods are currently available [3]. Wire localization of nonpalpable lesions on the day of surgery is the most common localization technique. However, this procedure has several limitations [4], including patient discomfort, risk of wire displacement, and fracture or transection before or during the surgical procedure, consequently resulting in operative delays and interference with the surgical approach [5,6].
Therefore, radioactive seed localization (RSL) and the use of a dye as a visual marker were introduced [4]. For example, iodine 125 (125I) RSL was developed by Luini et al. at the European Institute of Oncology in Milan in 1998 [7]. The seeds are placed internally, without external wires extruding from the skin surface; patient satisfaction is markedly enhanced, and there is no risk of wire dislodgement, migration, or transection with resultant loss of localization [3]. However, the patientŌĆÖs exposure to radiation and difficulty of repositioning after an initially wrong insertion are drawbacks.
To overcome these limitations, our institution has implemented a new localization technique using an absorbable retaining thread (ART; COBUILD, Goyang, Korea). The use of a guiding needle and ART has been approved by the Korea Food and Drug Administration. The ART needle is composed of a guiding needle with a cog polydioxanone thread, which has numerous barbs that become fixed inside the breast lesion. Therefore, the purpose of this study was to investigate the feasibility of ART needle localization of nonpalpable breast lesions before surgery.
Materials and Methods
All patients in this study agreed to the procedure, and informed consent for the procedure was obtained. We reviewed breast images and patientsŌĆÖ medical records to assess the feasibility of ART needle localization. This study was approved by the Institutional Review Board of our institution as a retrospective review.
From November 2014 to July 2015, we performed preoperative breast lesion localization in 275 cases. ART needles were inserted into 26 nonpalpable breast lesions under US guidance in 26 patients who planned to undergo surgery the next day at our institution. The mean age of patients was 52.0┬▒10.1 years (range, 34 to 71 years).
The initial histologic diagnosis of 24 breast lesions was made through a US-guided 14-gauge core needle biopsy at our institution or at an outside clinic. Seventeen breast lesions were initially diagnosed as invasive ductal carcinoma (IDC), six as ductal carcinoma in situ (DCIS), and one as fibrocystic change, which showed an imaging-pathologic discordance. Among the patients diagnosed with an IDC, five underwent neoadjuvant chemotherapy. The other two cases without an initial pathologic diagnosis showed suspicious US features, and excision was planned concomitantly with contralateral breast cancer surgery. ART needle localization was performed by one of two radiologists who had 1 and 15 years of experience, respectively, in breast imaging and interventions.
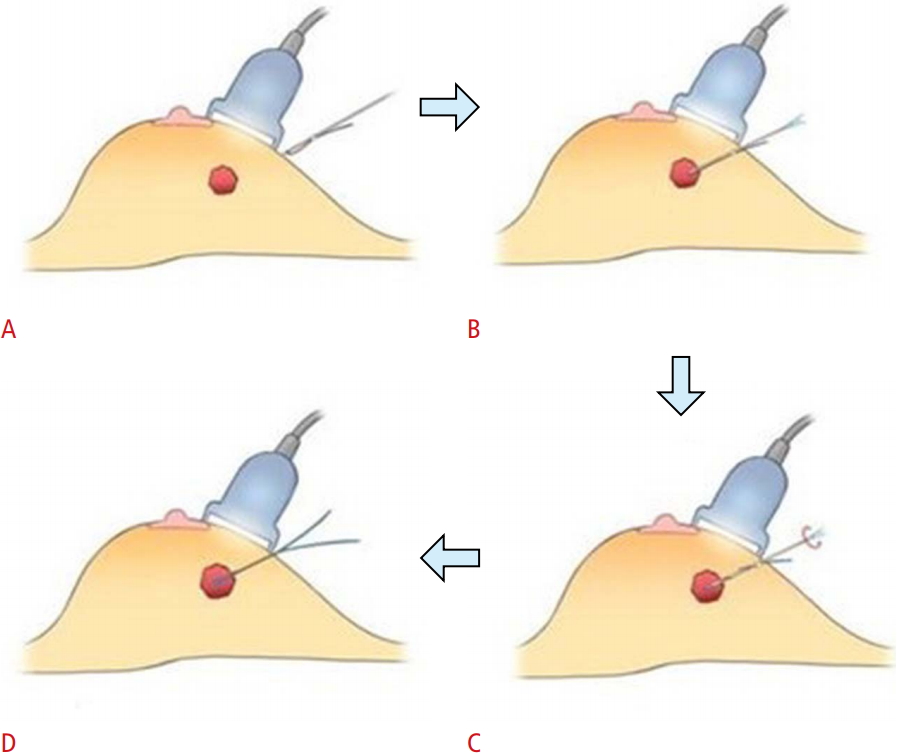
This procedure was performed as follows: after routine preparation with povidone iodine and local anesthesia, a 20-gauge guiding needle with an absorbable thread was inserted into the center of the breast lesion under US guidance (Fig. 1). The guiding needle was rotated to fix the thread inside the lesion and was subsequently removed (Fig. 2). The ART outside the skin was covered with gauze and taped. The procedure took approximately 5 minutes.
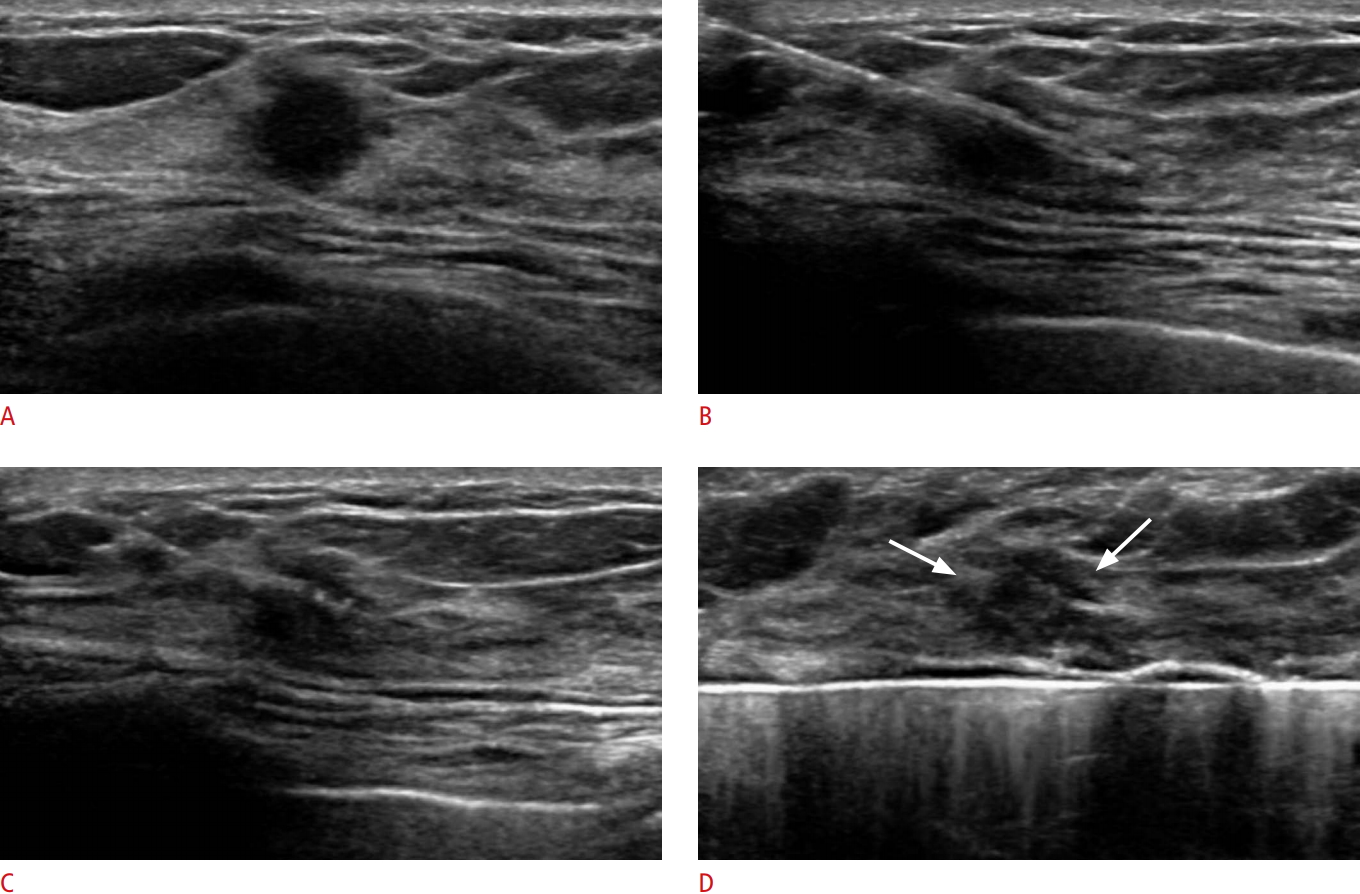
We confirmed the location of the thread by US immediately after performing ART needle localization (Fig. 3A, B). The localization was considered to be successful when the thread was shown within the lesion by US (Fig. 3C). After surgical excision, specimen mammography and/or US was also performed to assess the safety margin of the lesion (Fig. 3D). Complete excision was confirmed by a pathologist.
The primary outcome of this study was defined as the technical success rate of ART needle localization confirmed by US immediately after the procedure, and the secondary outcomes were defined as the rate of successful excision with clear margins on pathology and the complication rate. The complications of ART needle localization include significant hemorrhage, infection, and thread withdrawal or displacement.
Results
The longest diameter of the masses ranged from 0.4 to 2.7 cm (mean, 1.4┬▒0.7 cm) on US at localization and from 0 to 4.2 cm (mean, 1.4┬▒1.1 cm) on pathology. The final pathologic findings were 17 cases of IDC, including two patients with complete remission after neoadjuvant chemotherapy, one case of invasive solid papillary carcinoma, six cases of DCIS (including two cases of microinvasive DCIS), one case of atypical ductal hyperplasia, and one case of fibrocystic change.
The technical success rate, which was the primary outcome of the study, was 96.2%. The ART was successfully detected inside the mass in 25 of 26 cases on US immediately after the procedure. In one unsuccessful case, targeting the center of the mass on a transverse scan was difficult, because the mass had a longitudinal diameter of only 3 mm. In that case, the ART was located 1 cm away from the mass. Therefore, it was marked on the overlying skin with an oil-based pen, and the distance between the mass and the tip of the ART was reported to the surgeon.
The successful excision rate, which was a secondary outcome, was 100%. All breast lesions were successfully removed with the ART, verified with specimen radiography and/or US, and showed clear margins on the final pathologic findings. No complications related to ART needle localization were observed until the time of surgery.
Discussion
Improvements in imaging techniques have resulted in the increased detection of nonpalpable, clinically occult breast lesions that require localization before surgery [8].
The standard method for localizing breast lesions is wire localization [9]. The ability to accurately localize nonpalpable lesions with a wire needle revolutionized breast cancer surgery after it was first described in 1965 [10]. Although the wire needle localization technique is highly effective, it still has some disadvantages [11]. The procedure requires patients to first report to the radiology department for localization and await transportation to the operating room with a wire protruding from the breast, which is often uncomfortable and carries a risk of wire migration, leading to excessive tissue removal [10]. Additional complications and disadvantages include bleeding, infection, pneumothorax, and the wire being cut [12,13].
Several alternatives to wire needle localization exist, including RSL and the use of a dye, such as toluene blue, as a visual marker [5]. However, an obvious disadvantage of RSL compared to traditional wire localization is the patientŌĆÖs exposure to radiation. Furthermore, if a seed is not initially placed in a satisfactory position, it cannot generally be removed preoperatively. A second seed (or wire) must then be placed to accurately localize the lesion, with both subsequently retrieved surgically. In addition, a gamma detection probe is needed after the seed is localized [4]. To overcome these disadvantages, we applied a new device to localize nonpalpable breast lesions. Unlike RSL, ART needle localization is radiation-free and does not require additional equipment for finding the seed during surgery. The ART is a cog thread with tilted barbs to hook inside the tumor. Because the ART is a thread, we thought that it would have the potential to minimize the patientŌĆÖs pain or discomfort compared with wire needle localization. Therefore, we performed ART needle localization a day before surgery in patients who were scheduled to undergo surgery early in the morning, as they were suspected to have a higher risk of wire displacement and to experience more discomfort than patients who underwent wire localization on the day of surgery. It was expected that doing so would simplify the operating room scheduling and minimize the patientŌĆÖs inconvenience on the morning of surgery. In addition, the thread is made from bioabsorbable materials, such as polydioxanone, which was thought to be advantageous if the thread was cut accidentally. The rate of complete excision was 100% in our study, even though the surgeons were not used to ART.
ART needle localization was unsuccessful in only one of the 26 cases because of inaccurate targeting. This case indicated that the ART could move backward while being drawn off the guiding needle when it was lodged in the fat.
This study has several limitations. First, only patients who underwent localization on the day before surgery were selected. Therefore, selection bias may have been present. Second, the number of subjects was limited to only 26, which is too small a number for reliable overall generalization of the study results. Further studies are needed for continued assessment of this procedure.
In conclusion, ART needle localization showed high technical success rate (96.2%) in localization of nonpalpable breast lesions. Therefore, this procedure may be a feasible alternative to wire needle localization.

 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



