

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Thyroid nodules are common clinical problems. Although most thyroid nodules are benign and asymptomatic, some are symptomatic and require treatment. Surgery has long been the treatment of choice for patients with benign symptomatic thyroid nodules (BSTNs); however, since the introduction of the minimally invasive treatments for the management of BSTNs, current international practice guidelines [1-4] recommend minimally invasive methods (e.g., thermal or chemical ablation) as an alternative to surgery, as these methods can minimize the drawbacks of surgery and improve patients’ quality of life (QoL).
Among the minimally invasive methods currently employed to treat BSTNs, radiofrequency ablation (RFA) and ethanol ablation (EA) have been used widely to reduce nodule volume and improve nodule-related symptoms and cosmetic problems [5,6]. Although many previous studies, including randomized clinical trials and meta-analyses, have confirmed the effectiveness and safety of these procedures for the management of BSTNs [3,7-9], relatively little is known about the effects of these procedures on patient QoL. Regarding QoL after ablation treatment, several studies [10-12] have reported positive outcomes, whereas another study by Oddo et al. [13] showed the opposite results. In addition to causing compressive symptoms and cosmetic problems, thyroid nodules can affect other various aspects of daily life, including physical, social, and emotional well-being. Thus, whether ablation treatments improve thyroid-specific QoL should be verified in order to weigh the advantages and disadvantages appropriately.
Therefore, the primary purpose of this prospective, multicenter study was to evaluate the effects of RFA and EA on changes in thyroid-specific QoL in patients with BSTNs, and the secondary purpose was to evaluate the volume reduction ratio (VRR) and safety of these procedures.
Materials and Methods
Compliance with Ethical Standards
The protocol of this study was approved by the Ethics Committees of the Institutional Review Boards of the two participating centers (Asan Medical Center and Ajou University Hospital, institutional review board number: 2015-0608). Written informed consent was obtained from all patients before they underwent RFA or EA.
Participation
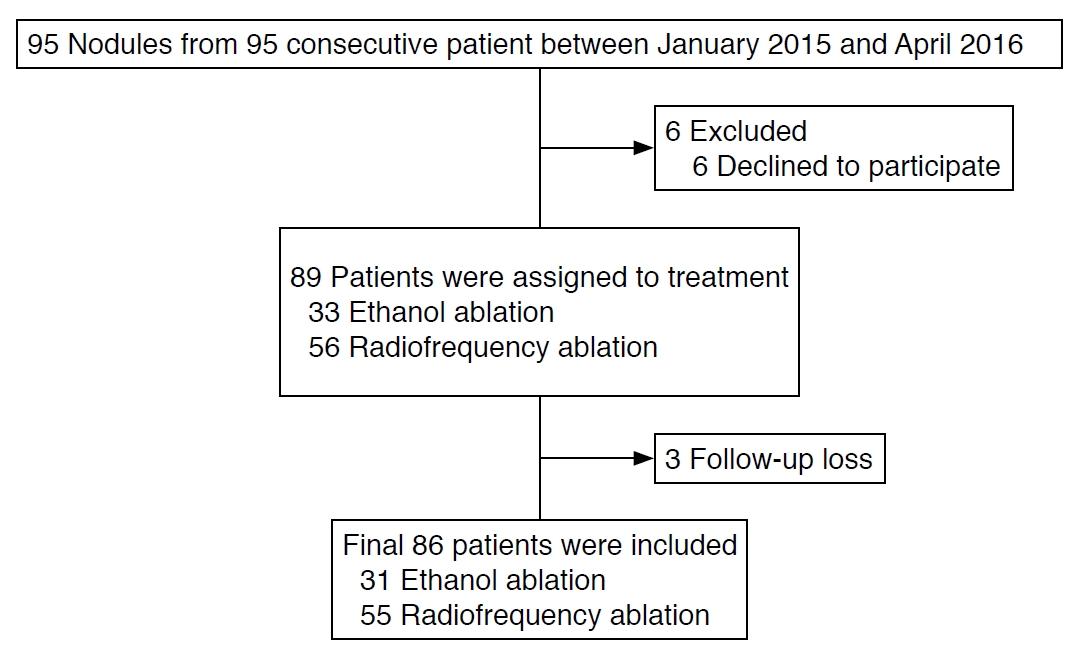
Between January 2015 and April 2016, 95 BSTNs from 95 consecutive patients were identified from the two participating centers (Fig. 1). After excluding six patients who declined to participate, 89 patients were treated with RFA or EA. After treatment, three patients were lost to follow-up before 6 months and were also excluded. A final sample of 86 patients with 86 BSTNs was included in this prospective study. RFA was performed for 55 BSTNs with a solid component ≥50% and EA was performed for 31 BSTNs with a solid component <50%.
The eligibility criteria for inclusion were as follows: (1) patients who reported symptoms or cosmetic problems due to a single thyroid nodule or a predominant thyroid nodule in a goiter, (2) benign cytology confirmed through the evaluation of at least two separate ultrasound (US)-guided fine-needle aspiration samples or core needle biopsies [14,15], (3) normal thyroid function tests, and (4) patients who were considering undergoing EA or RFA. The exclusion criteria were as follows: (1) patients who were younger than 20 years, (2) thyroid nodules with suspicious sonographic features, (3) abnormal thyroid function tests, and (4) pregnancy.
Preprocedural Assessment
All US systems were equipped with a high-frequency linear probe (5-14 MHz). Three orthogonal diameters-the longest diameter and two perpendicular diameters-were measured, and the volume of each nodule was calculated using the following equation: V=πabc/6 (where V is the volume, a is the longest diameter, and b and c are the two perpendicular diameters). The composition of each nodule was graded into four categories based on the proportion of the solid component: 1, solid (no obvious cystic content); 2, predominantly solid (cystic content ≤50%); 3, predominantly cystic (cystic content >50%); and 4, cystic (no obvious solid content).
Before the treatment, the physicians recorded a cosmetic score as follows: 1, no palpable mass; 2, no cosmetic problem but a palpable mass; 3, a cosmetic problem on swallowing only; and 4, a readily and always detected cosmetic problem. Patient-determined symptom scores were rated on a visual analogue scale from 0 to 10 as baseline data. Benign cytological results were confirmed by experienced cytopathologists according to the Bethesda classification system.
Assessment of QoL
Thyroid-specific symptoms and QoL in patients with BSTNs were evaluated using a thyroid-specific QoL questionnaire, which was translated into Korean and validated for patients with thyroid disease (Supplementary Table 1). Considering that patients with BSTNs often face unique QoL problems as compared with those other types of neck masses, assessment using a disease-specific QoL questionnaire was considered important.
The questionnaire evaluated the physical, psychological, and spiritual dimensions, with responses scored on a scale from 0 (none) to 4 (very severe). The QoL questionnaire consisted of 11 separate scales in the following aspects: goiter symptoms (11 items), tiredness (7 items), cognition (6 items), anxiety (6 items), depression (7 items), emotional susceptibility (7 items), impaired social life (4 items), impaired daily life (6 items), impaired sex life (2 items), cosmetic concern (6 items), and overall QoL (1 item). Since this study only included patients with normal thyroid function, the scales evaluating symptoms of hyperthyroidism and hypothyroidism were excluded. The QoL questionnaire was administered to patients before the procedure and 1, 6, and 12 months after treatment. Two clinical research coordinators administered the interviews and questionnaires.
Ablation Procedures
All procedures were performed by two experienced radiologists who had evaluated the preprocedural US images (J.H.B. and E.J.H. with 24 and 14 years of clinical experience, respectively, in evaluating neck US images and performing the procedure).
RFA was performed using an 18-gauge monopolar modified internally cooled electrode (VIVA, STARmed) with a 0.5, 0.7, or 1.0 cm active tip, as well as a radiofrequency (RF) generator (VIVA RF generator, STARmed) and a peristaltic pump (VIVA pump, STARmed). Under US guidance, the ablation needle was inserted into the nodule by the trans-isthmic approach, and ablation was performed using the moving-shot technique, with 30-70 W of RF power, depending on the sizes of the treated nodule and active tip. Ablation was terminated when the entire target lesion was covered with hyperechoic microbubbles.
EA was performed by inserting an 18-gauge needle via the normal thyroid tissue to minimize leakage of ethanol outside the cyst. After aspiration of cystic fluid, 99% sterile ethanol was injected through the same needle. The amount of injected ethanol was less than 50% of the aspirated fluid volume. After 5-10 minutes with the needle in place, the injected ethanol was removed completely, and the needle was withdrawn.
Procedure-related pain was graded into four categories and recorded. In RF procedures, the four categories were as follows: grade 0, RF power did not have to be turned off because the patient experienced no pain; grade 1, RF power was turned off once or twice to reduce pain levels; grade 2, RF power was turned off more than three times; and grade 3, RF procedure was incompletely terminated due to severe pain. In EA procedures, the four categories were as follows: grade 0, no pain or mild pain similar to the pain experienced during the lidocaine injection; grade 1, pain greater than the lidocaine injection, but not needing medication; grade 2, pain needing medication; and grade 3, EA procedure terminated before completion due to severe pain. Complications and side effects were defined according to the quality improvement guidelines of the Society of Interventional Radiology and a prior multicenter evaluation of complications. Each patient was monitored in the hospital for 2 hours after RFA and for 30 minutes after EA.
Follow-up and Outcome Assessment
US examinations were performed at 1, 6, and 12 months after RFA or EA. In the US examinations, changes in nodule size and volume were evaluated. The QoL questionnaire was administered during each visit, and improvements in patients’ symptoms and cosmetic problems were evaluated. Any adverse events occurring during the 12-month follow-up period were recorded.
Statistical Analysis
Categorical variables are presented as numbers and percentages, and continuous variables are expressed as mean±standard deviation. Linear mixed-effects modeling was performed for longitudinal data analysis. The model included group, time, and an interaction between group and time as the fixed effects. Patterns of covariance among repeated observations were modeled to account for correlations among observations for each subject, with covariance patterns selected from comparisons between models using the likelihood ratio test. The model parameter was obtained using the residual maximum likelihood estimation method, implemented with a Newton-Raphson algorithm. All P-values were two-sided, and a P-value <0.05 was considered to indicate statistically significant. Statistical analyses were performed using SPSS for Windows version 23.0 (IBM Corp., Armonk, NY, USA).
Results
Patient Demographics and Clinical Characteristics
The baseline clinical and treatment characteristics of the patients are summarized in Table 1. The mean longest size and mean volume of the index nodule were 4.2±1.5 cm and 21.6±22.1 mL, respectively. They showed no significant differences between the EA and RFA groups in the longest mean nodule size (4.1 cm vs. 4.3 cm, P=0.526) and mean nodule volume (22.0 mL vs. 21.3 mL, P=0.248). Of the 31 BSTNs that underwent EA, 23 (74.2%) were predominantly cystic and eight (25.8%) were cystic, and of the 55 BSTNs which underwent RFA, 30 (54.5%) were predominantly solid and 25 (45.5%) were solid. Of the 86 patients, 77 (89.5%) underwent one session of treatment and nine (10.5%, one EA case and eight RFA cases) underwent two sessions. The mean procedure-related pain was 1.0±0.7 during RFA and 0.0±0.2 during EA.
Treatment Efficacy
Table 2 shows changes in the size and volume of BSTNs over time after treatment. After the procedures, significant reductions in the mean volume of the ablated nodules were noted at 1-, 6-, and 12-month follow-ups (all P<0.001). In comparison between the EA group and RFA group, the mean VRR of the EA group was significantly higher than that of the RFA group at the 1-, 6-, and 12-month follow-ups (78.7%±16.1% vs. 49.1%±15.8%, P<0.001; 86.3%±21.7% vs. 73.0%±14.5%, P=0.002; and 90.9%±14.9% vs. 80.3%±12.4%, P=0.004, respectively).
After the procedures, both symptom and cosmetic scores decreased significantly at the 1-, 6-, and 12-month follow-ups (all P<0.001). The symptom scores were not significantly different between the EA group and the RFA group at any time point after the procedures. However, the cosmetic scores were significantly lower in the EA group than in the RFA group at the 1- and 6-month follow-ups (2.4±1.1 vs. 3.1±0.9, P=0.002 and 1.8±0.9 vs. 2.4±1.0, P=0.009, respectively); while there were no significant differences at the 12-month follow-up (1.8±1.2 vs. 1.9±0.8, P=0.443).
QoL at Baseline and Follow-up
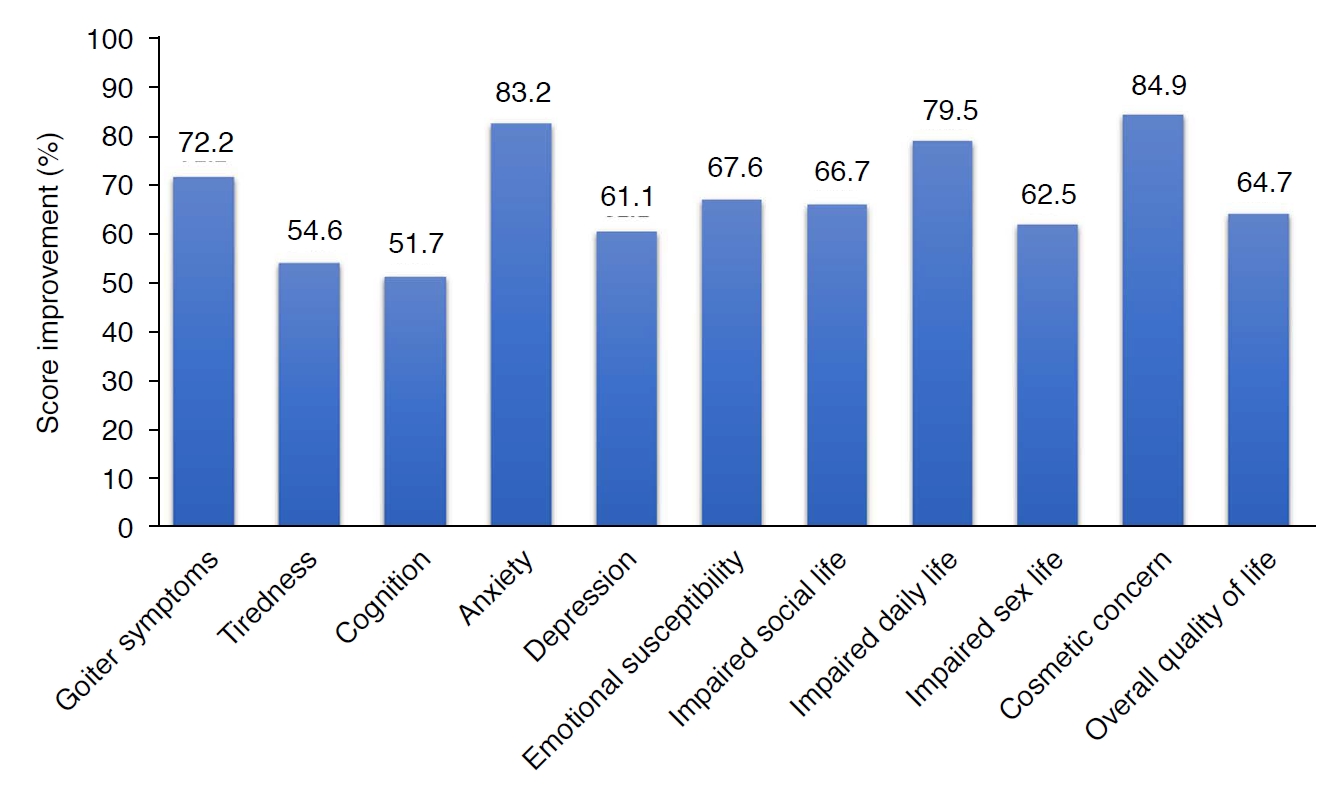
Table 3 shows the thyroid-specific QoL scores in these patients at baseline and 1, 6, and 12 months after treatment. The scores on each scale of the QoL questionnaire showed a significant improvement from the baseline to 1, 6, and 12 months after RFA or EA (all P<0.001). The overall QoL, which was scored from 0 (good) to 4 (poor), persistently improved from baseline to the 12-month follow-up over time (from 1.7±0.9 to 0.6±0.7). Fig. 2 shows the score improvement percentage for each scale. The scores for anxiety and cosmetic concerns showed an improvement of more than 80% (83.2% and 84.9%, respectively). In contrast, the scores of cognition, tiredness, and depression showed an improvement of about 50% (51.7%, 54.6%, and 61.1%, respectively).
Before the procedures, cosmetic concern scores were significantly higher in the EA group than in the RFA group (7.7±6.9 vs. 3.9±4.9, P=0.002), but there were no statistically significant between-group differences at the 1-, 6-, and 12-month follow-ups. Goiter symptom scores decreased more rapidly in the EA group than those in the RFA group at 1 month (2.4±3.1 vs. 6.5±7.2, P=0.002), but there were no significant differences at 6 and 12 months. Scores for tiredness, cognition, anxiety, depression, emotional susceptibility, impaired social/daily/sex life, and overall QoL during the follow-up period were not significantly different between the two groups (all P>0.05).
According to the baseline nodule volume, the patients were divided into two groups (small to medium, <20 mL; and large, ≥20 mL), and analyzed the anxiety scores between the groups. Patients with a baseline nodule volume larger than 20 mL had higher anxiety scores than patients with a baseline nodule volume less than 10 mL (8.8±6.3 vs. 10.4±7.1, P=0.295). However, this tendency did not have clinical significance.
Safety
Several patients who underwent RFA and EA reported mild pain at the treated sites, or pain radiating to the head, ear, shoulder, or teeth during the procedure. However, the pain was reduced when the generator output was reduced or turned off during ablation. All patients tolerated RFA or EA. There were no major complications, such as nerve injury or nodule rupture.
Discussion
This study prospectively evaluated changes in thyroid-specific QoL scores after RFA or EA in patients with BSTNs. Both procedures significantly improved all thyroid-specific QoL scales (all P<0.001) and reduced mean nodule volume by 80.3%-90.9% at the 12-month follow-up.
US-guided minimally invasive treatments, such as RFA or EA, have been proposed for the management of patients with BSTNs during the past two decades [1,2]. Current international practice guidelines generally recommend RFA for nodules with a solid component ≥50% and EA for nodules with a solid component <50% [2,16-18]. However, it is not well known whether the effects of these treatments eventually improve QoL in these patients. In this study, thyroid-specific QoL, including all the physical, psychological, and spiritual dimensions, significantly improved after RFA or EA. Goiter symptoms resolved more rapidly in the EA group than those in the RFA group at the 1-month follow-up (2.4±3.1 vs. 6.5±7.2), but there were no differences at the last follow-up (3.3±3.4 vs. 3.1±7.2). Other symptom scales also improved persistently in both groups. By contrast, a previous study by Oddo et al. [13] reported no significant improvement in QoL scales after RFA, except for the "general score," which improved after 3 months. They explained that the cause of less improvement seemed to have been due to the low VRR, which was <50% in most patients. In comparison, in the present study, it was possible to achieve a much higher VRR at the 12-month follow-up (90.9%±14.9% in the EA group and 80.3%±12.4% in the RFA group) and all thyroid-specific QoL scales in both groups improved after treatment. Sufficient VRR should be achieved by trained operators using a unified protocol and similar devices to improve thyroid-specific QoL after the procedure.
The scores for items that were directly related to nodule size such as anxiety and cosmetic concern showed a greater improvement (83.2% and 84.9%, respectively) than the others. Moreover, patients with larger baseline nodule volume tended to have higher anxiety scores (8.8±6.3 vs. 10.4±7.1, P=0.295). However, the scores for items that were relatively uncorrelated with nodule size such as cognition, tiredness, and depression showed relatively less improvement (51.7%, 54.6%, and 61.1%, respectively). This study did not include patients with functioning nodules, and it appears that the items that showed relatively less improvement were related to thyroid function rather than nodule size. The inclusion of patients with functioning nodules might change such results.
Surgery is a long-established therapeutic option for BSTNs [19,20]. However, the cost of thyroid surgery, the risk of temporary or permanent complications, and the effect on QoL remain relevant concerns [12,21]. Regarding QoL after surgery, several previous studies demonstrated that surgery may not lead to an overall improvement in QoL in patients with BSTNs [22,23]. In a prospective observational study by a German group of surgeons [23], QoL scores did not change in most patients after surgery, while 21%-30% showed improvements and 14% showed a deterioration in QoL. Regarding these issues, Yue et al. [12] compared the QoL scores of propensity score-matched patients with benign thyroid nodules that were treated with RFA or surgery. In their study, patients treated with RFA had significantly better QoL than patients treated with surgery for general health, vitality, and mental health at a 6-month follow-up, while the QoL scores were significantly improved on role-emotional and mental health in both groups. Further studies of direct comparison with surgery are necessary for these issues.
QoL is one of the key considerations when deciding the clinical management for patients with thyroid lesions [24]. US-guided minimally invasive treatments, such as RFA or EA, are also promising for QoL improvement in patients with thyroid cancer. In a recent prospective study by Morris-Wiseman [25], thyroid cancer patients with postoperative permanent hypoparathyroidism had significantly lower QoL, with nearly three to five times as many general symptom-related problems, as patients without hypoparathyroidism. Several studies have reported that RFA showed good clinical outcomes, with better QoL, compared with surgery in patients with recurrent thyroid cancers in the dissected neck [26-28]. Chung et al. [27] also demonstrated that RFA is effective for local tumor control, even for tumors invading the airways. In addition, several recent studies have shown that RFA is highly encouraging in terms of low morbidity and recurrence rates and high thyroid-cancer-specific QoL scores in patients with low-risk papillary thyroid microcarcinoma [26]. Although all treatments have potential risks, clinicians managing thyroid nodules should have a multitude of sources to consult for optimal personalized management. Patients should be fully informed regarding QoL before selecting a treatment option.
This study had several limitations. Although a VRR of more than 80% was achieved after EA or RFA within 12 months, long-term follow-up results are necessary to evaluate the actual clinical impact of these ablation treatments on QoL. In addition, this study did not include patients with functioning nodules. Because proper management of functioning nodules remains controversial, further studies are necessary to achieve better outcomes with fewer side effects.
In conclusion, both RFA and EA are safe and effective in thyroid-specific QoL as well as improving the reduction of nodule volume in patients with BSTNs.
 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



