

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Imaging guidance is a key factor in conferring both effectiveness and safety for numerous interventional procedures. Among the multitude of available imaging techniques, ultrasonography (US) and computed tomography (CT) are the most commonly used in guiding abdominal interventions [1-4]. However, US stands alone as the only true real-time method and remains the most preferred guiding tool, with several advantages over CT and magnetic resonance imaging (MRI), especially given its high accessibility. Yet, in comparison to sectional imaging, the lack of contrast administration previously limited the effectiveness of conventional US guidance. In clinical practice, there were numerous cases in which grayscale US did not suffice for guidance, an illustrative example being non-visible, isoechoic lesions, which in the past required a referral for a contrast-enhanced CT-guided procedure [5,6].
US Contrast Agents and Harmonic Imaging
The successful introduction of microbubble US contrast agents (UCAs) in the past decades has enabled the real-time contrast-enhanced assessment of various tumors, parenchyma, or complex pathological structures [7,8]. Not only do microbubbles enhance the diagnostic capacities of US, but they also enable interventional procedures performed either for diagnostic (aspiration, punctures, biopsies) or therapeutic (drainages, ablations) purposes [5-10].
The mechanisms, particularities, and advantages of various UCAs are well documented and are not the focus of the current review [5-7,11]. However, the distinction between the two most frequently used contrast agents, SonoVue (Bracco, Switzerland) and Sonazoid (GE Healthcare, Amersham, UK), is of particular interest. SonoVue microbubbles are composed of sulfur hexafluoride gas with a phospholipid shell. The contrast agent is metabolized by the liver and further exhaled by the lungs, providing the typical arterial (20-30 seconds), portal (45-90 seconds), and late (>180 seconds, but less than 10 minutes) phases. In contrast, Sonazoid (currently approved only in Japan, Korea, and Scandinavia) consists of microspheres of perfluorobutane stabilized by a monomolecular membrane of hydrogenated egg phosphatidylserine, embedded in an amorphous sucrose structure. Unlike SonoVue, Sonazoid is taken up by Kupffer cells in the post-vascular phase, leading to an additional post-vascular phase (Kupffer phase, 5 to 30 minutes after the injection), providing extremely stable images suitable for repeated scanning and interventions, and thus removing the time-constraint generated by rapid contrast clearance. Moreover, the Sonazoid bubbles have a relatively narrow size distribution, are very robust-allowing for high mechanical index (MI) scanning (MI=0.2-0.3) and are not deterred by the use of higher US frequencies [5,12].
Applications: Intravascular, Intracavitary, and Combined Use
The UCA is manually administered through an intravenous line, most commonly via an antecubital vein, followed by a 10 mL flush of 0.9% normal saline. To avoid disrupting the microbubbles, UCAs should be administered relatively slowly. A contrast-enhanced ultrasonography (CEUS)-compatible US system with contrast agent-specific software that uses conventional low-MI imaging is required. Contrast enhancement can be shown on a split-screen display with a conventional B-mode image and a low-MI CEUS image presented either side-by-side, or on a single-screen display where the CEUS image is presented as a color overlay on the conventional B-mode image [5,6,9,11,13].
The technique for intracavitary administration of UCAs is similar to the technique used for focal lesions. The key differences consist of the UCA dosage and injection modality. According to the most recent European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) Guidelines published in 2020, the dose range recommended for extravascular (intracavitary) CEUS is 0.1-1 mL SonoVue diluted in 10 mL of 0.9% saline [7]. The dose of UCA depends on the type of cavity (physiological or non-physiological cavity) and the aim of the study. To emphasize (or exclude) a connection between two cavities, the anatomy of fistulas, or pleuro-peritoneal communication, a higher dose (1-2 mL) is necessary. Conversely, to delineate the cavity of a collection (abscess, pseudocyst), only a few drops of UCA suffice to avoid artifact formation. The route of administration is either through a previously placed drainage tube or through a needle (18 G, Chiba), which is inserted into the cavity or excretory systems (biliary or renal) [5,9,11,13-15]. To address specific clinical questions (e.g., liver abscess), a combination of these two modalities, in any order, can be used. When performing similar examinations successively, it is necessary to disrupt the microbubbles by deploying a higher-energy US pulse compared to normal B-mode levels before repeating the UCA administration [9,11,15]. Other than local pain during the injection, no other adverse reactions have been documented in multiple clinical studies [11].
Benefits of CEUS Guidance
CEUS has the capacity of emphasizing the macrovasculature and, above all, the microvasculature of the parenchyma and tumors. Besides the well-accepted use in the detection and characterization of various tumors, the use of this technique has enabled the delimitation of areas with abnormal or absent vasculature [5,9,11,13]. These unique features are valid for both focal parenchymal lesions (e.g., tumors, abscesses) and post-procedural scars (e.g., post-ablation necrosis, embolization). The potential benefits of CEUS guidance are presented in Table 1.
Technique of Intravascular CEUS-Guided Interventions: Preprocedural versus Real-Time
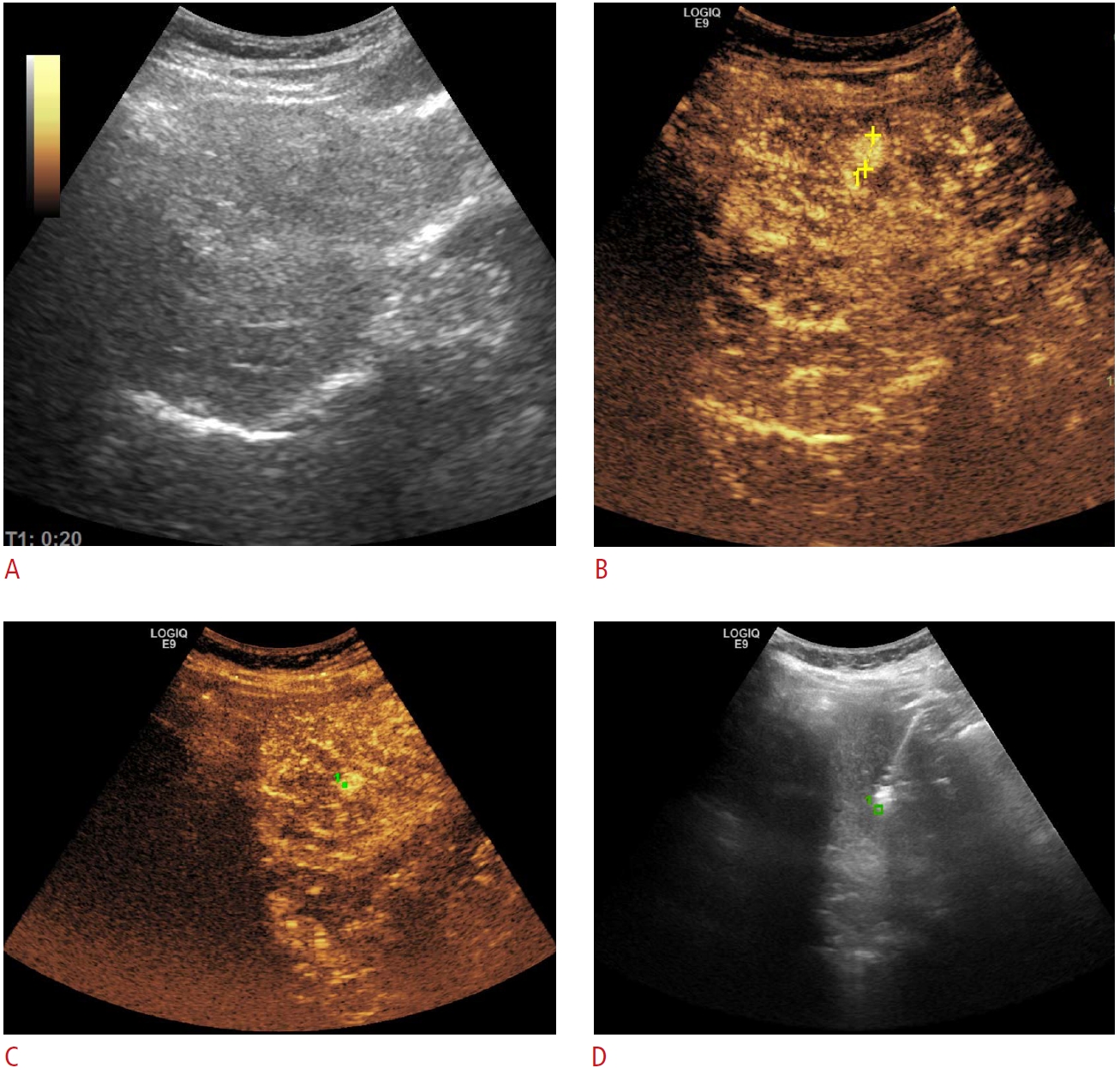
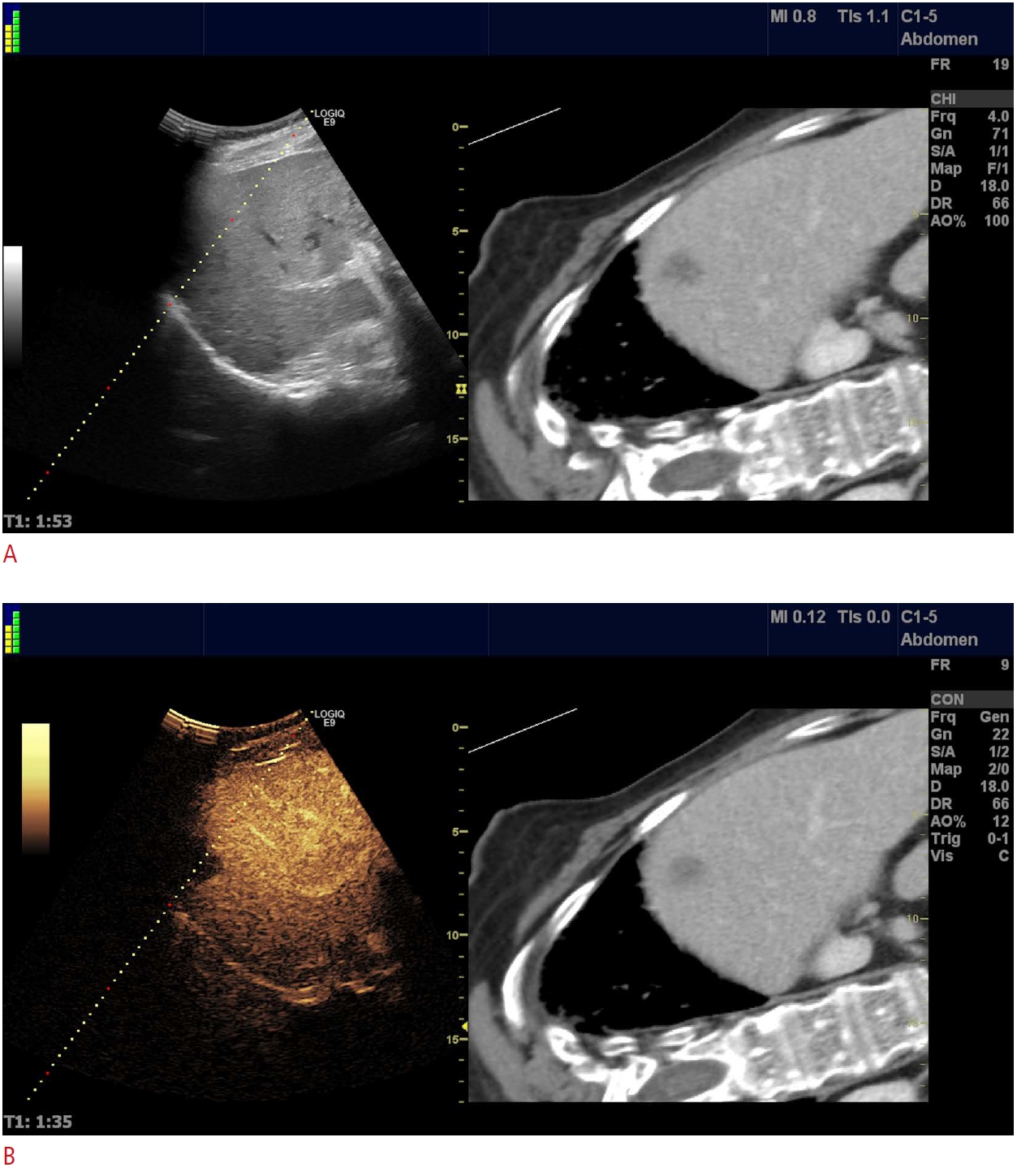
The timing of the UCA injection can add a nuance of precision to CEUS-guided interventions. In most cases, preprocedural CEUS is enough to increase the spectrum of relevant information about the point of interest (morphology, necrotic areas). It facilitates a more accurate procedure plan, which will subsequently be performed in grayscale mode. Furthermore, by utilizing GPS navigation, the operator can mark the desired target during the enhancement phase and expand the benefits of preprocedural CEUS to real-time guidance (Fig. 1) [13,16].
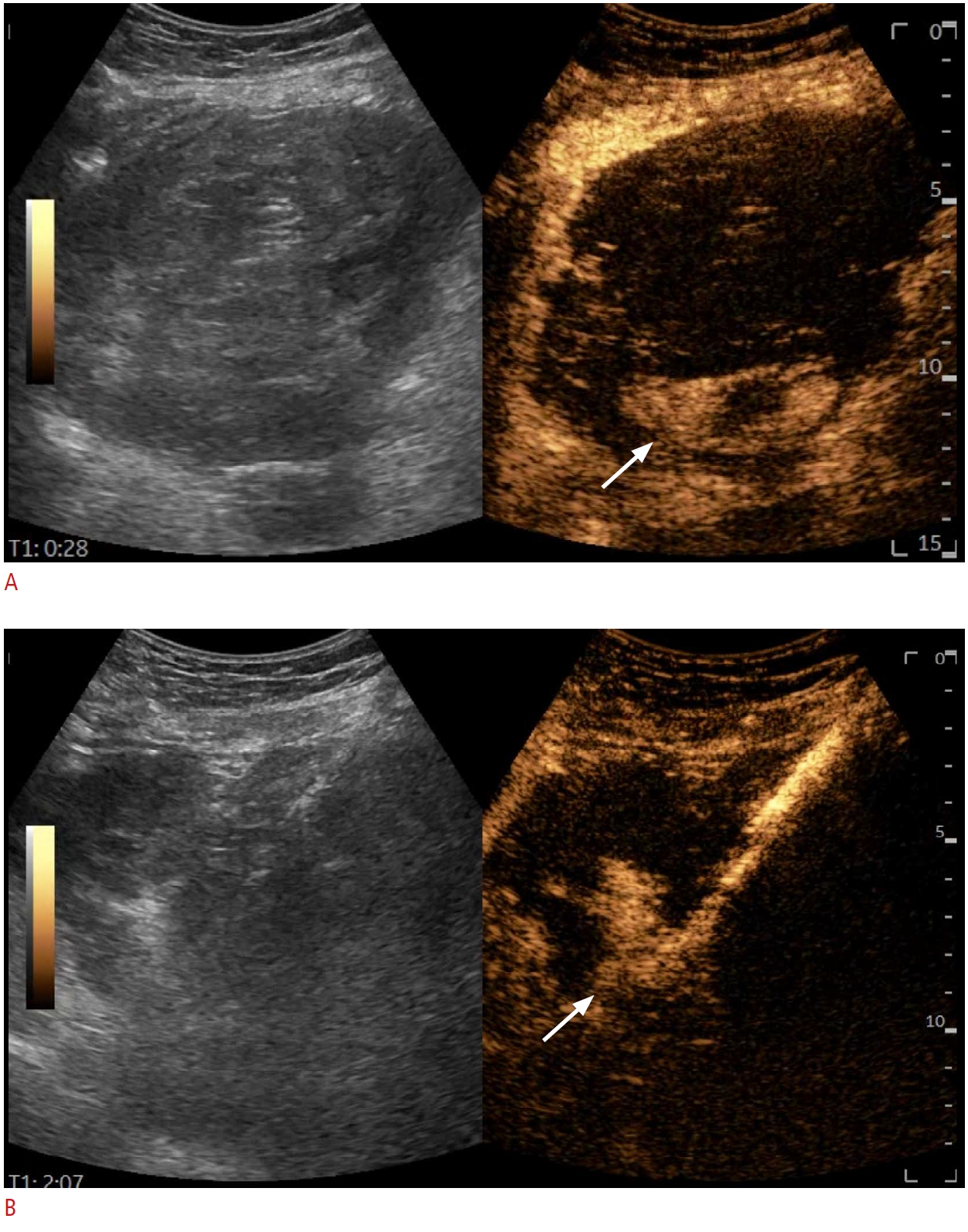
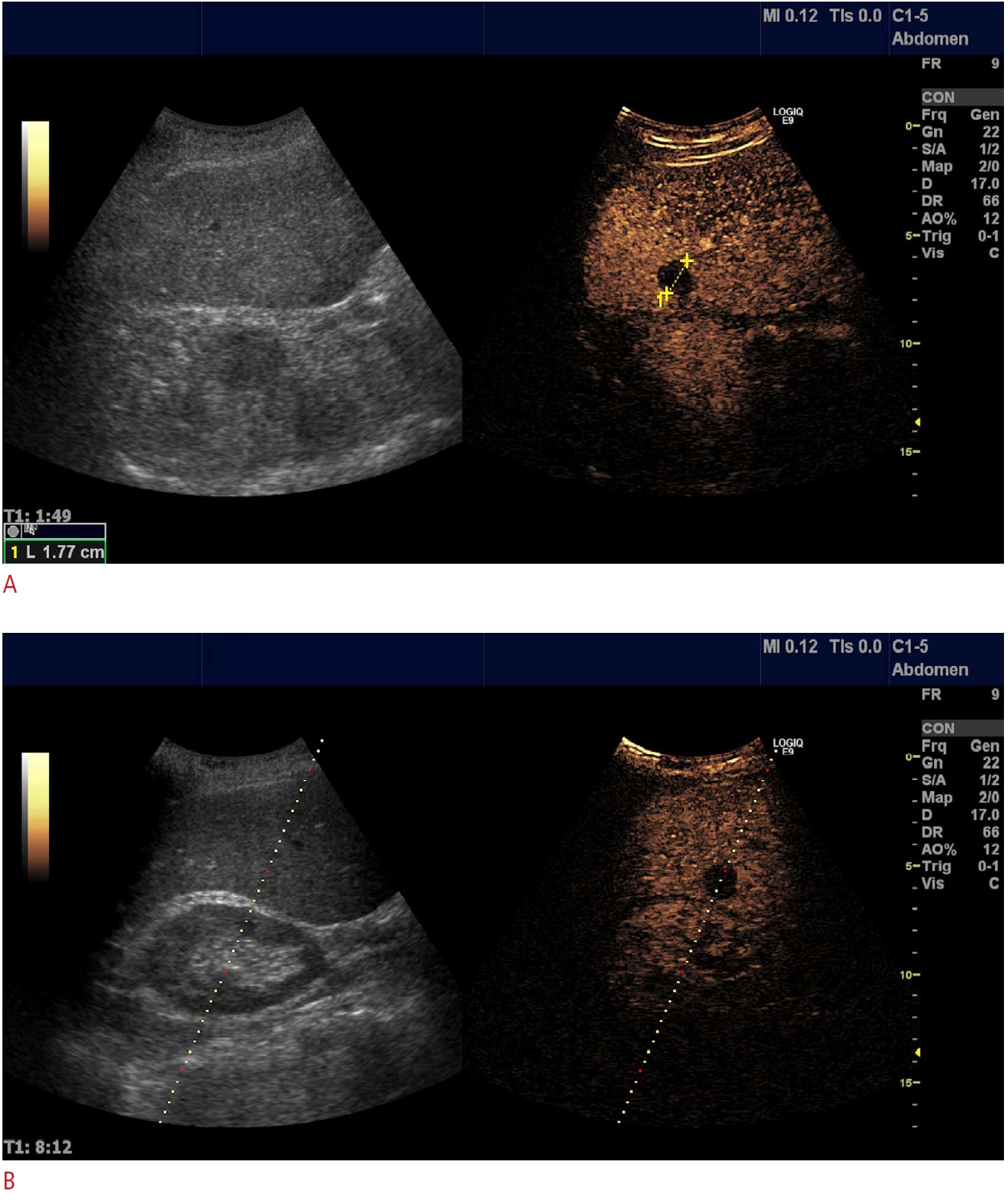
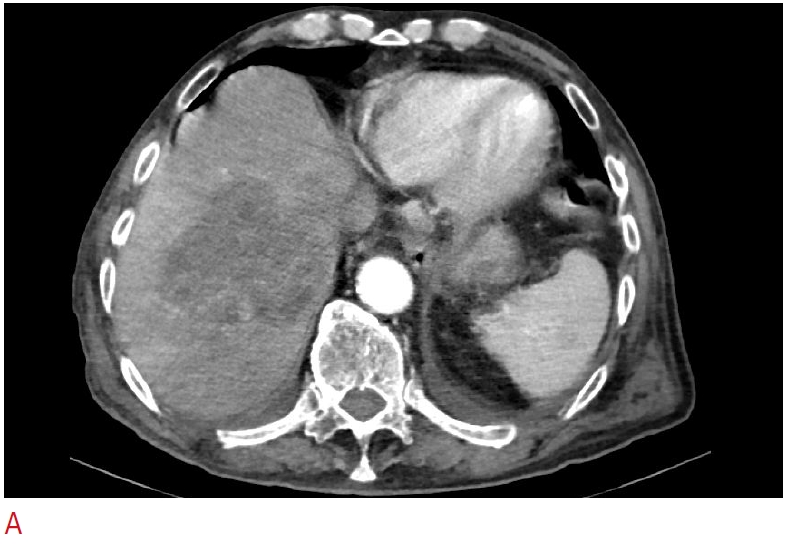
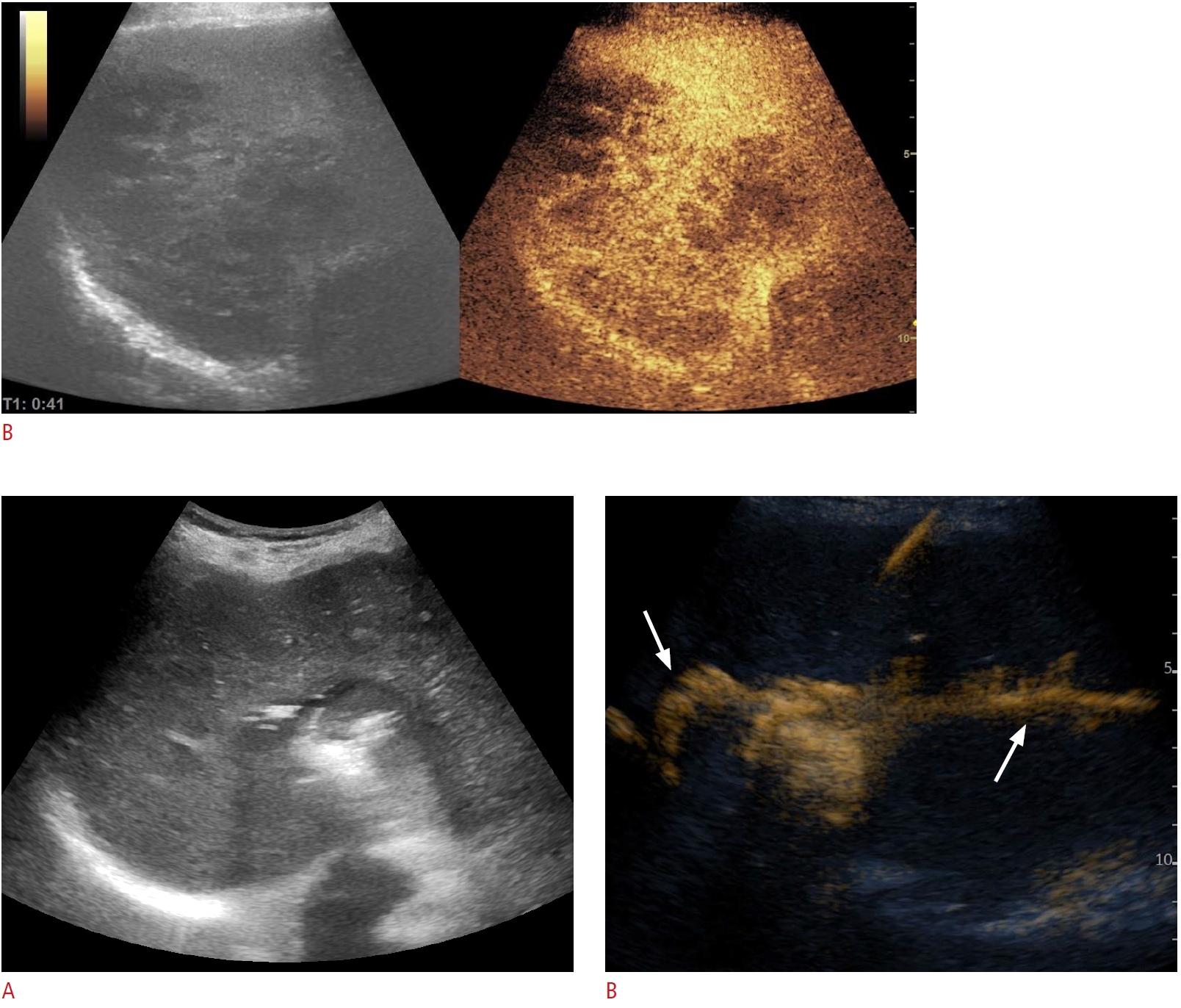
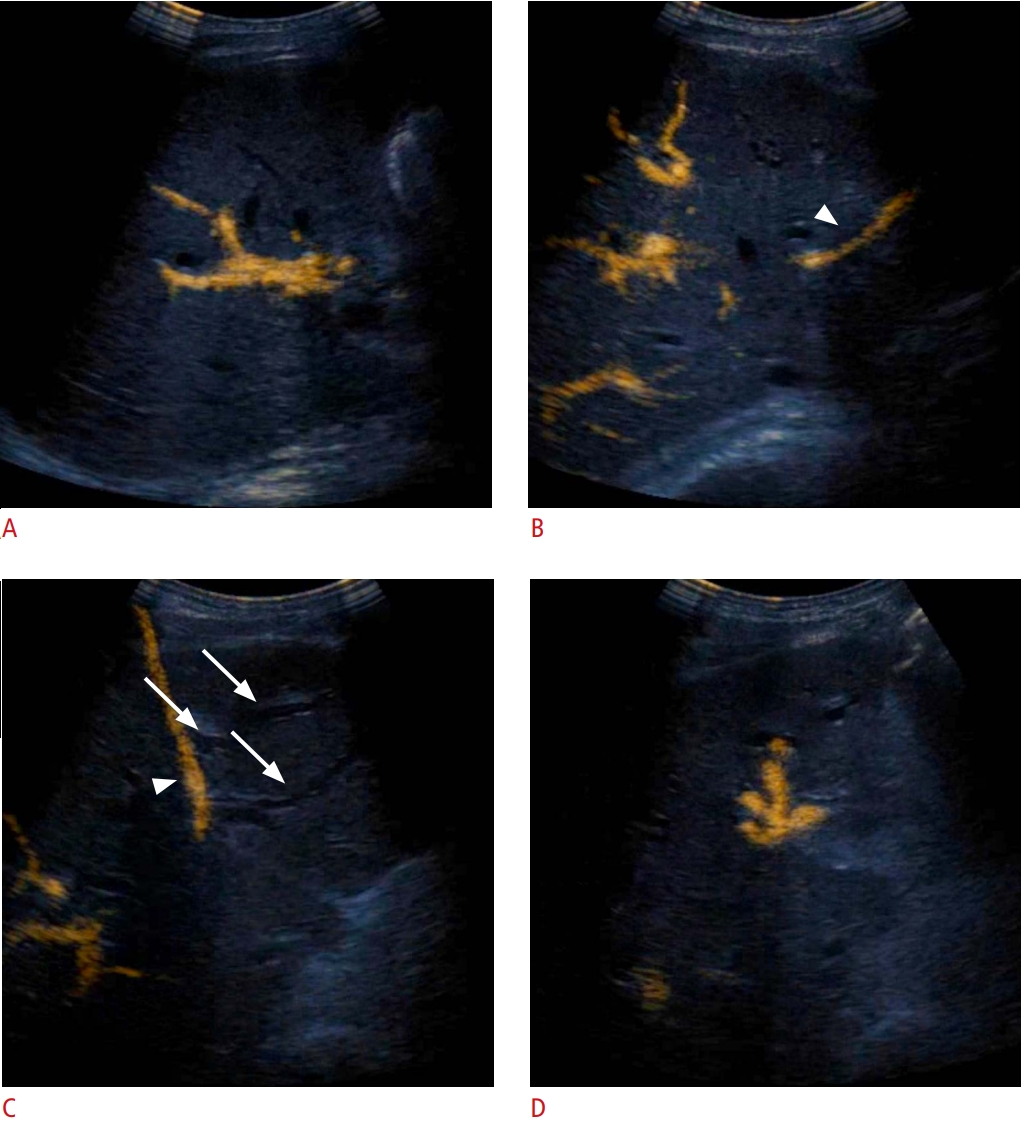
However, real-time CEUS is the most precise manner of guidance, although it requires a more advanced skillset. It was also the first technique utilized at the time of the use of the first-generation UCA Levovist [17]. There are numerous sequences in which the UCA injection can be synchronized with the puncture, depending on the type of procedure. Typically, in the case of SonoVue, the 4.8 mL vial is subdivided into up to four doses. The first dose is used for pre-planning and mapping, while the subsequent doses are used for real-time guidance. In between the first and second doses, preparations can be performed (sterilization, drape placement, and local anesthesia). Real-time guidance is most frequently required in two clinical scenarios: to avoid large areas of tumoral necrosis (Fig. 2) and to locate obscure B-mode lesions. Consequently, for liver tumors, the moment of needle insertion should be synchronized with the desired outcome: arterial phase (10-30 seconds after the UCA injection) to avoid undesired areas of puncture or to target hypervascular lesions not seen in B-mode US and the portal (30-120 seconds) and parenchymal (120-600 seconds) phases for targeting metastasis that is inconspicuous in grayscale images (Fig. 3) [5,9,13,18,19].
The use of real-time CEUS can sometimes become a significant challenge. When the biopsy is performed in the late phase, which can last up to 7 minutes, time allows for multiple passages. On the contrary, guidance in the 30-second arterial phase can become a race against the clock, allowing no room for error. This limitation can be overcome by using needle guides and attentive planning during the mapping CEUS [15,20,21]. There might be concerns about needle visibility during CEUS. Yet, in most cases, this does not represent a real issue, and the use of a split-screen view resolves needle visualization.
Upon advancing through the learning curve, each user can make slight variations of the working algorithm, to better suit personal preferences.
CEUS-CT/MRI/Positron Emission Tomography-CT Fusion
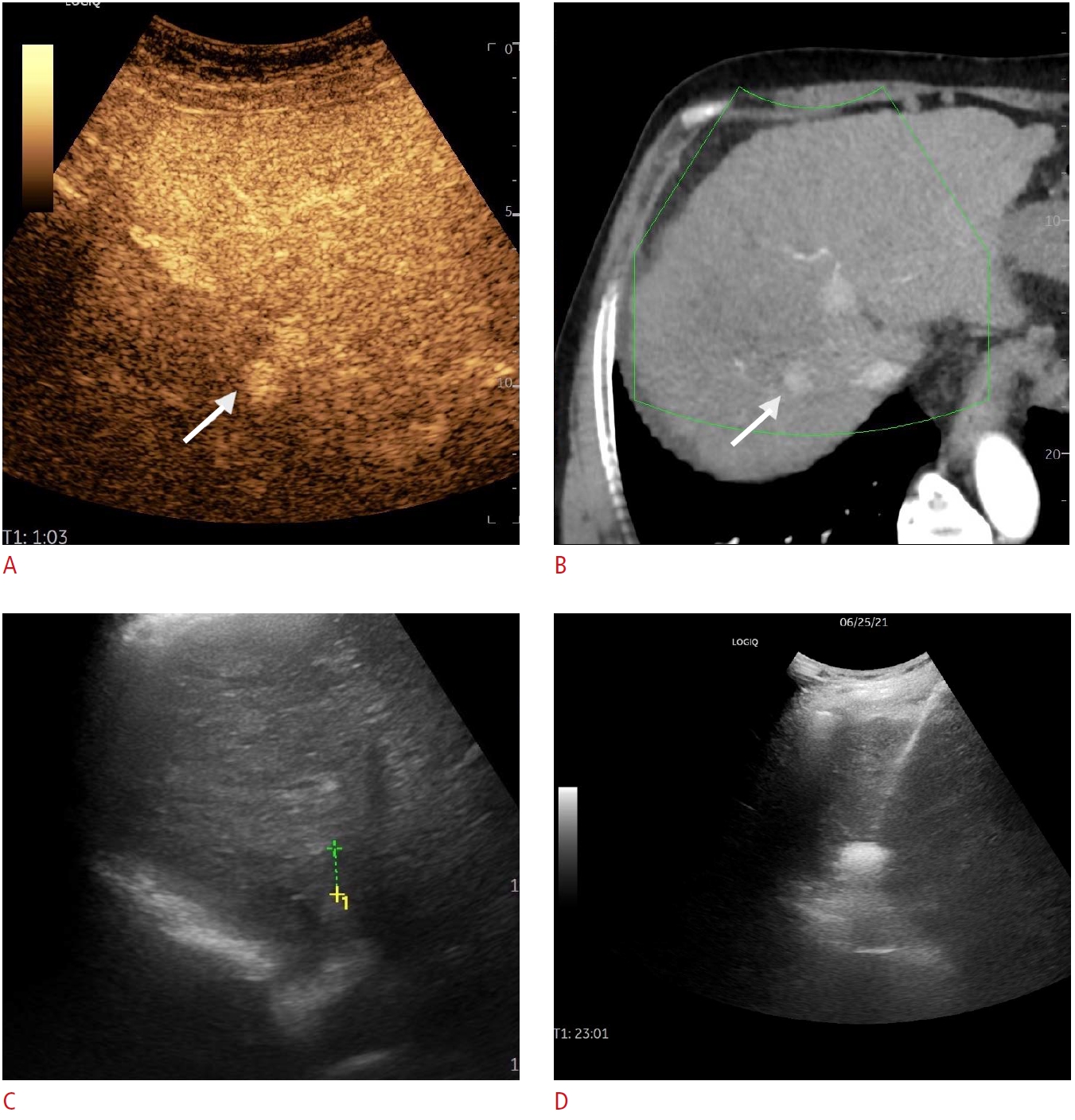
Conventional B-mode US may overlook some lesions, especially if they are isoechoic or small. Fusion imaging increases the detection rate and is of great help in guiding percutaneous interventions (biopsies, ablations) on the liver. However, the sensitivity of fusion imaging is not always perfect, with some small nodules still remaining undetected [22]. When fusion imaging is insufficient, adding CEUS in the US-CT fusion guidance increases the conspicuity of some lesions, which might prove useful, especially in small nodules (Figs. 4, 5) [23].
The introduction of CEUS guidance and other complementary methods has changed how we think and plan interventional procedures. With recent technical developments, new algorithms will most likely emerge. Is there also a paradigm shift in interventional ultrasound after the introduction of these methods? The following paragraphs will address this question.
CEUS as a Tool to Increase the Efficacy of Percutaneous Biopsy
Despite dramatic improvements in imaging- and biomarker-based diagnosis in recent years, percutaneous biopsy still plays a pivotal role in providing the most accurate diagnosis. With all the advantages offered by US guidance, the overall sensitivity of this method in the diagnosis of tumors remains around 90% [13].
The potentially added value of CEUS in tumoral diagnosis through percutaneous biopsy may be related to several factors.
Improving Lesion Targeting
Using CEUS, the conspicuity of focal lesions (liver, kidney, and pancreas) is improved. This is true for both small, isoechoic lesions and large, isoechoic infiltrating tumors. CEUS guidance might be used in the arterial phase for hypervascular lesions not seen in grayscale US, such as small hepatocellular carcinomas (HCCs) in patients with cirrhosis, or the late phase for liver metastases [13]. With the use of the new UCAs like Sonazoid, it became possible to target the liver lesions in the Kupffer phase (20-30 minutes after contrast injection), practically eliminating the time-constraint to perform the biopsy [12]. The use of CEUS before a biopsy may identify new lesions with an easier pathway for biopsy. The added value of CEUS is probably of most relevance when lesions are embedded in an already modified parenchyma and are otherwise difficult to detect (HCC nodules in liver cirrhosis, lung cancer in atelectatic parenchyma, or abscesses in pneumonia) [24-26]. Not least, CEUS is also relevant for patchy tumoral organ involvement, such as lymph nodes or prostatic adenocarcinoma [13].
Abstaining from Biopsy When It Is Unnecessary
Although sectional imaging methods have a good sensitivity for diagnosing focal liver lesions, there are some circumstances (i.e., small lesions, especially hemangiomas) where the lesions may be misinterpreted or have a nonspecific pattern. In those cases, CEUS performed before the biopsy may change the diagnosis and thus avoid the biopsy [6,13,27,28].
The improved accuracy of CEUS-guided liver and thoracic biopsies versus conventional B-mode guidance has been reported in numerous papers [16,19,26,27,29]. Intending to avoid necrosis, CEUS-guided biopsy increases the diagnostic yield of the pathology report by up to 20% in liver biopsies [6]. Furthermore, the CEUS-guided puncture of poorly visible or invisible liver lesions has a success rate of 86% to 100% [6,19,30]. In advanced chronic liver disease, CEUS adds a 20% increase to the overall sensitivity and a 30% sensitivity increase for lesions with poor conspicuity on B-mode US [26]. Moreover, using Sonazoid, it was reported that CEUS guidance significantly increased the technical success rate by 26% and the rate of successful single puncture attempts by 20% compared to B-mode guidance [31].
Adding CEUS to US-CT fusion guidance increases the visibility of lesions, with 77.8%-93.8% of initially invisible lesions being detected [32,33].
In the biopsy of thoracic lesions, in comparison to grayscale US guidance, CEUS guidance increases the sensitivity of the procedure from 80.3% to 96.3%, while decreasing the complication rate (3.7% vs. 18.2%). This advantage was achieved by a better distinction between tumor and atelectasis and higher performance in detecting necrotic tissue [29].
Renal and other retroperitoneal tumors may grow very large, with frequent and extensive necrosis, rendering them suitable for CEUS guidance [13]. Preliminary reports have demonstrated the good feasibility of CEUS-guided biopsies, with diagnostic sensitivities of 96% in renal tumors and large retroperitoneal and intraperitoneal tumors (18% higher than US-guided biopsies) [34,35].
CEUS-Guided Biopsy in Clinical Practice
Although CEUS-guided percutaneous biopsy was shown to add 10% to 15% to the procedural success rate, its use in daily clinical practice is currently limited. A multicentric Italian study showed that real-time CEUS guidance was used in only 2.6% of 3818 biopsies. In order of frequency, CEUS-guided biopsy was used to avoid necrosis (39.8% of cases), to improve the target visibility (33%), and to target invisible lesions (27%). Approximately one-fourth (25.2%) of cases had a previously non-diagnostic biopsy. There are several reasons for the limited use of CEUS-guided biopsy in clinical practice, as follows: good experience for operators performing US-guided biopsy even for difficult cases; the routine use of CEUS in the diagnostic workup with valuable information already available at the time of biopsy; and the technical difficulty of real-time guidance, which is challenging for deep and small lesions [36].
In conclusion, while CEUS guidance is not required for every case of focal lesion biopsy, there are many clear-cut scenarios in which enhancing the lesion enhances the overall results. Although routine use may increase costs and procedure time without adding significant value [21], a judicious approach can maximize the outcome.
CEUS in Percutaneous Drainage Procedures: Abscesses, Biliary Tree, and Nephrostomy
Percutaneous drainage procedures are probably the latest realm conquered by CEUS guidance, adding refinement to what was previously a supplement to B-mode. However, since the field is still emerging, the present data remain scarce and unorganized, mostly consisting of case reports and small series.
Abscess Drainage
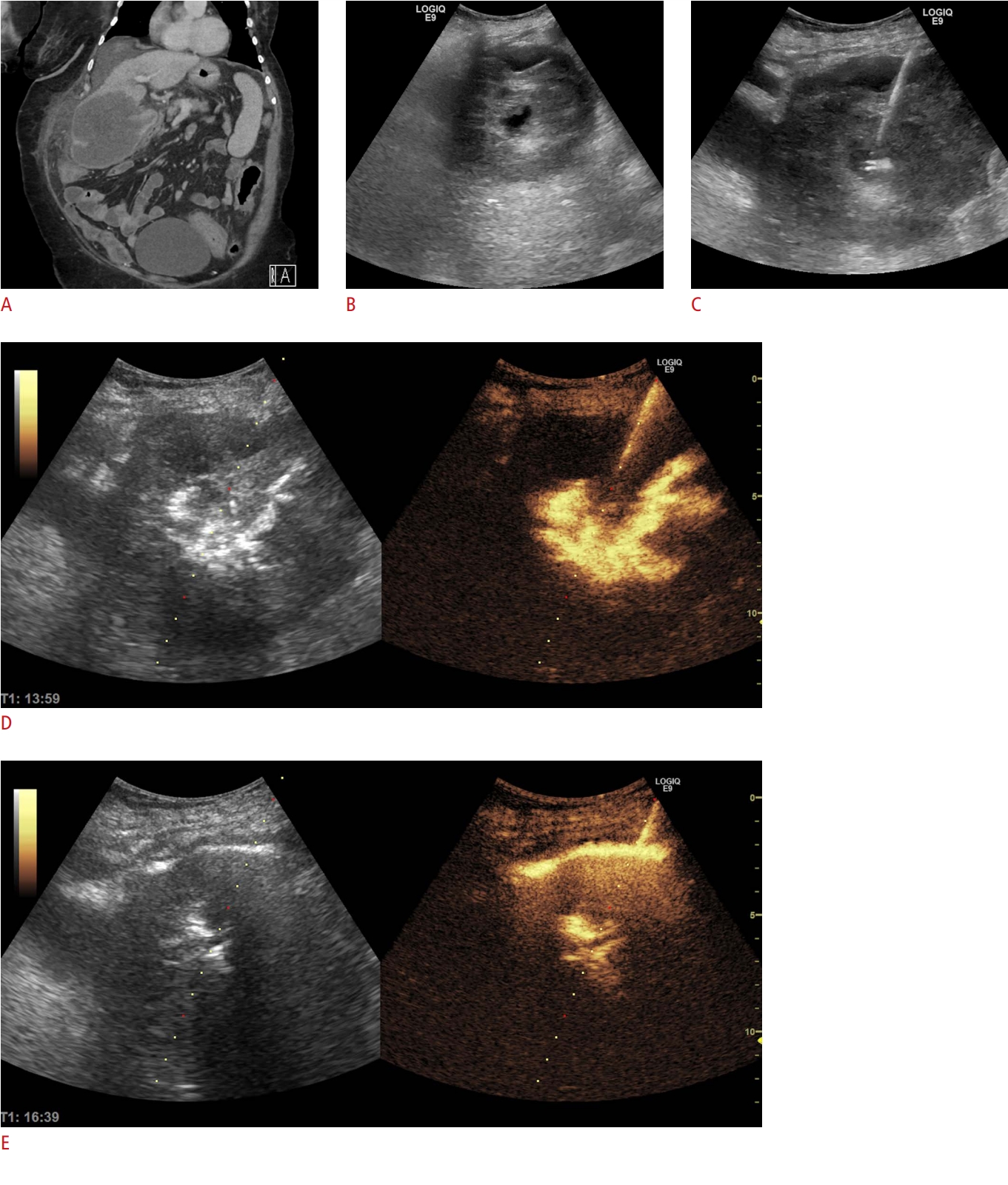
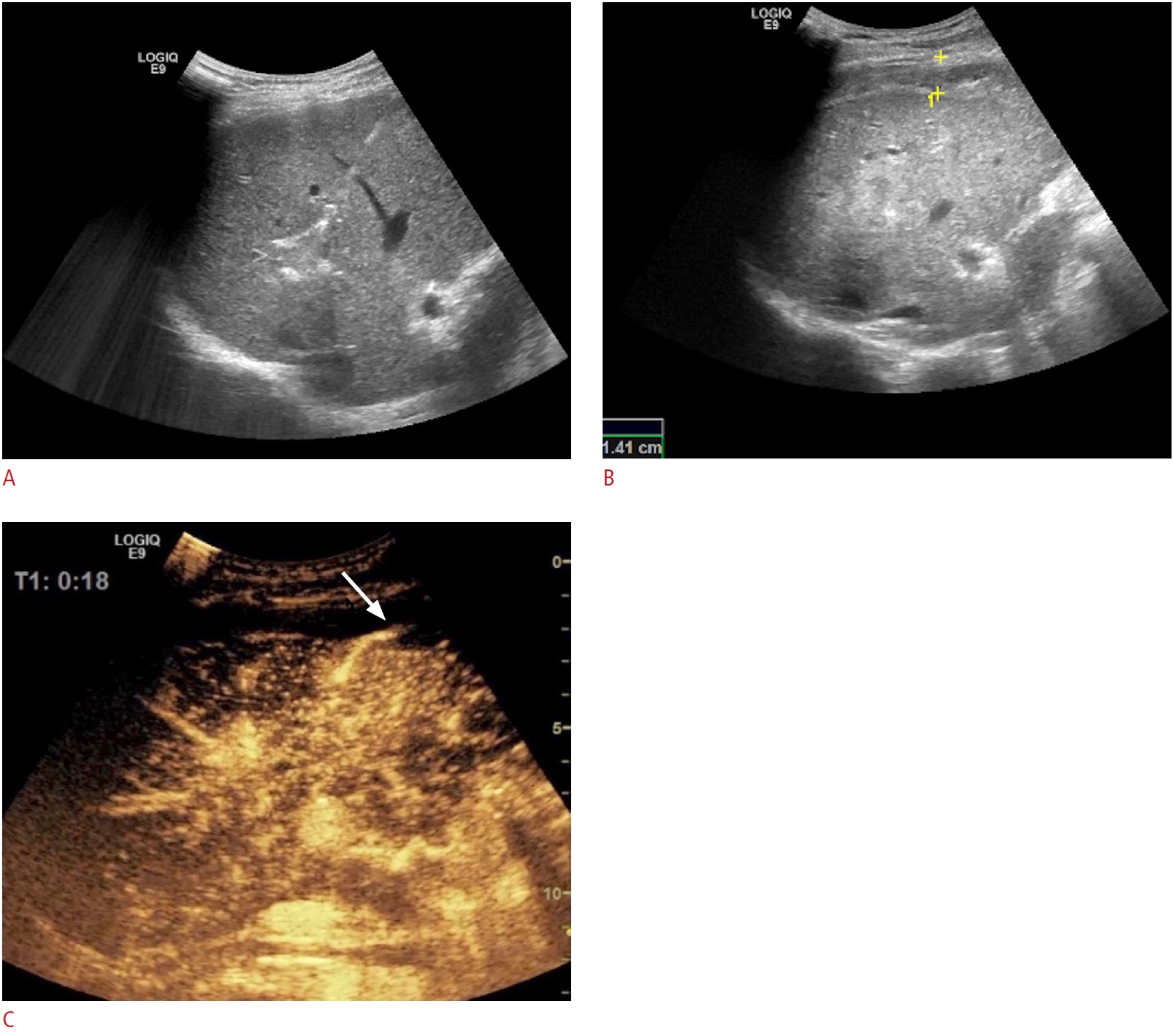
Abscesses can take numerous shapes and sizes. Thus, their correct management can become a significant challenge especially with regards to exactly when and where to place the tube to achieve the best results. The best timing can be selected using serial evaluations to refrain from premature or unnecessary procedures (without the toll of multiple CT scans) as proven by recent data [37] and illustrated in Fig. 6. The grayscale appearance might often be misleading, as septa, multilocularity, or fistulas can detract from therapeutic success [6]. In this situation, intracavitary CEUS can help, as it provided additional information regarding undrained areas or communication with anatomical structures (Figs. 7, 8) in almost 50% of the cases in the largest available series on the topic [38].
Biliary Tree: Cholangiography and Drainage
There is a purported role of CEUS in characterizing the biliary tree, being a bedside, non-irradiating alternative to fluoroscopy. Once the biliary tree is percutaneously accessed, the injection of a small, diluted amount of UCA can confirm the needle location, define the map of drained regions through a quick scan of the entire liver parenchyma (Fig. 9), aid tube positioning, and/or detect prior aberrant lesions (bile leaks, fistulas, etc.), with similar results to those of fluoroscopy. Choosing between conventional fluoroscopy and CEUS cholangiography is, to this point, a matter of debate and, ultimately, a matter of personal preference. While image interpretation is not as straightforward and the spatial resolution might be lower, CEUS has the advantage of accessibility. The method can be performed in the US department, by the same operator who performed the drainage placement and can lead to a quick fine-tuning of the tube. There are no clear-cut data in favor of either of the two available methods [6,39].
Kidney: Pyelogram and Nephrostomy
In kidney obstruction and drainage, CEUS plays a similar role as discussed in the biliary tree section. It provides a viable alternative to fluoroscopy, both in dilated and non-dilated pelvises, as well as in evaluating therapeutic success and stent patency [40-42]. Furthermore, it appears to be a valuable tool in evaluating the success rate of percutaneous nephrolithotomy [43]. Not least, pre-kidney puncture CEUS can delineate abnormal vascular patterns, thereby theoretically decreasing the complication rate.
CEUS-Guided Tumor Ablation
In the context of thermal ablation, CEUS falls into three categories: before, during, and after ablation [6]. The clinical benefits of using CEUS before ablation are as follows:
- Better delineation of the tumor size (in up to 56% of cases, the lesions were larger) and shape (in up to 49% of cases, the lesions were more irregular) [44]; this will translate into a higher complete necrosis rate and a lower complication rate when compared to B-mode US planning [44]
- Increasing the detection rate in patients with HCC (from 57% to 96%) [45]
- Revealing further ablation targets missed on conventional US examinations in up to 13% of cases with liver metastases [46]
- In 75% to 98% of cases, CEUS was reported to visualize and guide ablation of HCC that was previously invisible or inconspicuous on conventional US imaging [6].
In the second setting, several studies have reported the technical success rate for CEUS-guided percutaneous thermal ablation. The clinical scenarios for which CEUS guidance is useful during ablation are target lesions detected on contrast-enhanced CT or contrast-enhanced MRI and not visible on US, improvement of conspicuity of the target lesion, and depiction of a viable area inside nodules with either incomplete ablation after previous treatment or local tumor progression [2,47].
CEUS performed during ablation is challenging, especially in patients with HCC (the contrast medium rapidly washes out of the liver in the arterial phase, the quality of the image is insufficient, and the tip of the ablation needle has a poor echogenicity in CEUS mode). In this situation, we suggest the use of CEUS fusion with contrast-enhanced CT or MRI since it can depict invisible or inconspicuous nodules on the conventional US [48]. More importantly, the use of fusion techniques for inconspicuous lesions resulted in similar results as conventional US guidance for clearly visible lesions [49].
Lastly, CEUS is also a valuable clinical tool after therapy (Fig. 10). On one hand, it can be used immediately after ablation to detect incomplete ablations and allow retreatment within the same session in up to 50% of cases [50]. This feature is of particular importance since the residual tumor rate preferably should be as low as 0% [51]. On the other hand, when used as a follow-up evaluation tool, CEUS provides similar accuracy as CT or MRI for individual ablation targets.
CEUS in the Detection of Hemorrhagic Vascular Complications in Interventional Procedures
Albeit rare, some hemorrhagic vascular complications during or after US-guided interventions have been described. CEUS is an excellent tool for immediate detection and subsequent treatment planning (Fig. 11). The CEUS appearances of various hemorrhagic vascular complications after tumor ablation are depicted in Table 2.
Conclusion
The addition of CEUS to the interventional US armamentarium can offer substantial benefits ranging from preprocedural planning to real-time guidance and follow-up. There are numerous applications of contrast enhancement in clinical practice, from assisting biopsies, drainage procedures, and ablations, to post-procedural follow-up and detecting complications. The decision to use CEUS, as well as the timing and route of UCA delivery, makes a valuable contribution to the precision of the procedure. As the realm of USguided interventional procedures is ever-expanding, the judicious use of CEUS can provide a critical extra step in ensuring therapeutic success.

 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



