

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Radiofrequency ablation (RFA) is a curative treatment option for hepatocellular carcinoma (HCC). It is recommended for patients with very early-stage or early-stage HCC without optimal indications for surgery or transplantation [1]. The treatment outcomes after RFA are affected by tumor location. For example, although debate continues, subcapsular tumors have been considered problematic for percutaneous RFA (PRFA) [2]. However, some studies have shown that the results of RFA for subcapsular HCC are comparable to those for non-subcapsular HCC [3-7]. Conversely, subphrenic tumors, a subtype of subcapsular HCC, are still considered challenging to ablate via PRFA because of technical difficulties. Although some supportive skills, such as artificial ascites or pleural effusion, reduce the local tumor progression (LTP) rate after PRFA for subphrenic HCC [8-10], many studies have reported that subphrenic tumor location is a significant risk factor for LTP after PRFA [3,11,12]. Surprisingly, a previous study has reported that peritoneal seeding was found in up to approximately 10% of patients after ultrasound (US)-guided PRFA for subphrenic HCC [12].
Laparoscopic RFA (LRFA) has been attempted to overcome the technical difficulty of PRFA for subphrenic HCC, as it has various advantages over PRFA in terms of technical merits and survival outcomes [13]. A recent study showed that LRFA for treating subphrenic HCC had high technical efficacy and a very low LTP rate [14]. Therefore, it is postulated that LRFA would show better treatment outcomes than would PRFA for subphrenic HCC. However, to the authors’ knowledge, no study has directly compared the therapeutic outcomes between LRFA and PRFA for subphrenic HCC.
Therefore, this study aimed to compare the treatment outcomes of LRFA with those of PRFA for subphrenic HCC.
Materials and Methods
Compliance with Ethical Standards
This retrospective study was approved by the Institutional Review Board of Samsung Medical Center (2021-06-086), and the requirement for informed consent was waived.
Patients
This study used a longitudinal hospital registry from a single tertiary referral hospital. Patients who underwent either PRFA or LRFA as primary HCC treatment between January 2013 and December 2018 were included. In total, 1,816 patients were treated with PRFA. Among them, 1,565 were excluded for the following reasons: HCC treatment history (n=1,164), loss to follow-up after 1 month (n=35), other concurrent malignancy (n=160), multiple HCCs (n=32), HCC size of >3 cm (n=22), and tumor size of <1 cm (n=152). Tumor size was measured in the sequences that showed the best conspicuity of the tumor in dynamic enhanced liver magnetic resonance imaging (MRI). If the tumor had low signal intensity on the hepatobiliary phase, that sequence was preferred, and the longest diameter of the tumor was measured on either axial or coronal images. Two radiologists reviewed the computed tomography (CT) and MRI scans obtained before RFA and reached a consensus on the tumor location (subphrenic or non-subphrenic). Finally, 221 patients were further excluded because the HCC had a non-subphrenic location. Subphrenic tumors were defined as those abutting the diaphragm. Tumor size was defined based on the longest diameter on CT or MRI. Finally, 30 patients treated with PRFA for subphrenic HCC were included.
LRFA was performed in 124 patients. Among them, 84 were excluded for the following reasons: HCC treatment history (n=74), other concurrent malignancy (n=2), multiple HCCs (n=6), HCC size of >3 cm (n=1), and advanced HCC with bile duct invasion (n=1). The pretreatment images were also reviewed, and 17 patients were excluded due to tumors with a non-subphrenic location. Finally, 23 patients treated with LRFA for subphrenic HCC were included. Fig. 1 shows the flow diagram of patient selection. The HCC diagnosis was based on current clinical guidelines [15].
Percutaneous RFA
Planning US was performed by interventional radiologists to assess whether PRFA was feasible using fusion imaging (Volume navigation, LOGIQ E9, GE Healthcare, Chicago, IL, USA) of B-mode US and pretreatment CT/MRI, obtained within 1 month prior to the procedure [16]. Fusion imaging was routinely used for treatment planning regardless of lesion conspicuity. When PRFA was considered feasible, it was attempted by the same radiologists, who had more than 3 years of experience in RFA for hepatic tumors.
Radiofrequency electrodes were inserted under fusion imaging guidance; direct tumor puncture was avoided when the tumor was located in the anterior liver dome to prevent peritoneal seeding. Based on the tumor size and location, the choice was made to use an active tip length-adjustable internally cooled tip (Proteus RF Electrode, STARmed, Goyang, Korea), an internally cooled wet tip, a kind of perfusion electrode with various active tip lengths (Jet-tip, RF Medical, Seoul, Korea), or clustered separable electrodes with an internally cooled tip with different active tip length (Octopus Electrode, STARmed). To achieve a sufficient ablative margin, peripheral tumor-puncturing or no-touch RFA was preferred when using multiple electrodes or overlapping ablation when using a single electrode. The radiologist ensured that the index tumor was completely covered in the RFA zone based on US findings. The tract was cauterized during electrode removal.
Laparoscopic RFA
LRFA was considered after planning US when the subphrenic HCC location appeared technically challenging for PRFA. When both PRFA and LRFA were feasible, the treatment method was determined by the radiologist. LRFA was performed by one of three radiologists while the patient was under general anesthesia. The surgeons introduced three or four trocars through the subcostal and subumbilical areas. The patients’ positions were manipulated to insert the radiofrequency electrode in the appropriate direction. A single electrode (Proteus RF Electrode, STARmed) or clustered separable electrodes (Octopus Electrode, STARmed) were used.
When the subphrenic tumors were broadly attached to the anterior liver capsule, they were well visualized on laparoscopy. The radiofrequency electrodes were inserted in parallel under laparoscopic guidance [14]. Whenever needed, overlapping ablations were performed for complete ablation with a sufficient ablative margin. Direct tumor puncture was avoided (video clip). Laparoscopic US (Aloka Inc., Tokyo, Japan) was also used for tumors focally attached to the liver capsule; thus, the tumors were not visualized on laparoscopy. The liver capsule was cauterized on top of the index tumor based on laparoscopic US findings for tumors not visible on laparoscopy, which facilitated accurate electrode placement. The electrode’s position in relation to the index tumor was assessed using laparoscopic US. The RFA zone was monitored to ensure that it was large enough to cover the entire tumor using laparoscopy and US. The tract was ablated during electrode removal.
Treatment Response and Complications
Treatment response and complications were evaluated using contrast-enhanced CT on the day of the RFA. Treatment was considered technically successful if the RFA zone completely covered the index tumor on CT images [17]. A second RFA session was attempted within 24 hours after the first RFA session if technical success was not achieved. Technical efficacy was assessed on a 1-month follow-up CT or MRI scan. Major complications were defined as events that led to substantial morbidity and disability that increased the level of care, resulted in hospital admission, or substantially lengthened the hospital stay. All other complications were considered minor [17].
Follow-up
Follow-up contrast-enhanced CT/MRI was performed 1 month after initial treatment, every 3-4 months during the first 2 years, and every 4-6 months thereafter. Chest radiography, serum alpha-fetoprotein level measurements, and liver function tests were also performed. LTP was defined as the appearance of tumor foci at the edge of the ablation zone [17]. If recurrence, including LTP, intrahepatic distant recurrence (IDR), and extrahepatic metastasis (EM), occurred during follow-up, the multidisciplinary team decided on a suitable second-line treatment.
Comparison of Therapeutic Outcomes
The length of the ablation zone was measured in 3-dimensions on immediate post-RFA CT. The maximum (Dmax) and minimum (Dmin) diameters of the ablation zone were measured from axial CT images and the longest vertical diameter (Dv) from coronal or sagittal images. The ablation volume was calculated using the formula for an ellipsoid lesion: ablation volume=π (Dmax×Dmin×Dv)/6 [18]. The ratios of the longest diameter and volume of ablation zone to those of the tumors were compared between the PRFA and LRFA groups.
Therapeutic outcomes, including LTP, IDR, EM, disease-free survival (DFS), and overall survival (OS), were compared between the two groups. DFS was defined as the time from the day of ablation to recurrence or death. OS was defined as the time from the initial treatment to death or the last follow-up date before April 30, 2021.
Statistical Analyses
Demographic and clinical characteristics between the groups were compared using the t test, Wilcoxon rank-sum test, chi-square test, or Fisher exact test, as appropriate. Kaplan-Meier survival curves and the log-rank test were used to compare the cumulative LTP, IDR, EM, DFS, and OS rates. Statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA). Statistical significance was set at P<0.05.
Results
Baseline Characteristics
The baseline characteristics of the patients, which are summarized in Table 1, were not significantly different between the PRFA and LRFA groups. Liver function, assessed using the Child-Pugh class or albumin-bilirubin grade, was not significantly different between the two groups. The serum levels of alpha-fetoprotein and protein induced by vitamin K absence-II were also not significantly different. More than 70% of the patients had hepatitis B virus-related liver disease, and the cause of liver disease was not significantly different between the two groups. The tumor size and location (Couinaud segment) were also not significantly different. The characteristics of the ablation technique are summarized in Table 2. They were not significantly different between the PRFA and LRFA groups.
Technical Success and Efficacy of RFA
In the PRFA group, a residual unablated tumor was noted in one patient (3.3%) on the immediate post-RFA CT images. The second RFA session was performed on the same day, which led to successful local tumor control. Technical efficacy was achieved in 30 patients (100%). Four of the 23 tumors in the LRFA group were indistinguishable on laparoscopy. These tumors were localized using laparoscopic US, and RFA was conducted. Both technical success and efficacy were achieved in all 23 patients (100%).
Ablation Zone
The median longest diameter of the ablation zone was 4.1 cm (range, 2.8 to 5.5 cm) in the PRFA group and 4.7 cm (range, 3.3 to 6.0 cm) in the LRFA group. The median volume of the ablation zone was 18.4 cm3 (range, 7.6 to 44.5 cm3) in the PRFA group and 28.7 cm3 (range, 8.4 to 43.5 cm3) in the LRFA group. The ratios of the longest diameter or the volume of the ablation zone to those of the tumors in both groups are summarized in Table 3. The ablation zone was significantly larger in the LRFA group than the PRFA group in comparison to the tumor.
Comparison of Therapeutic Outcomes
Cumulative LTP rate
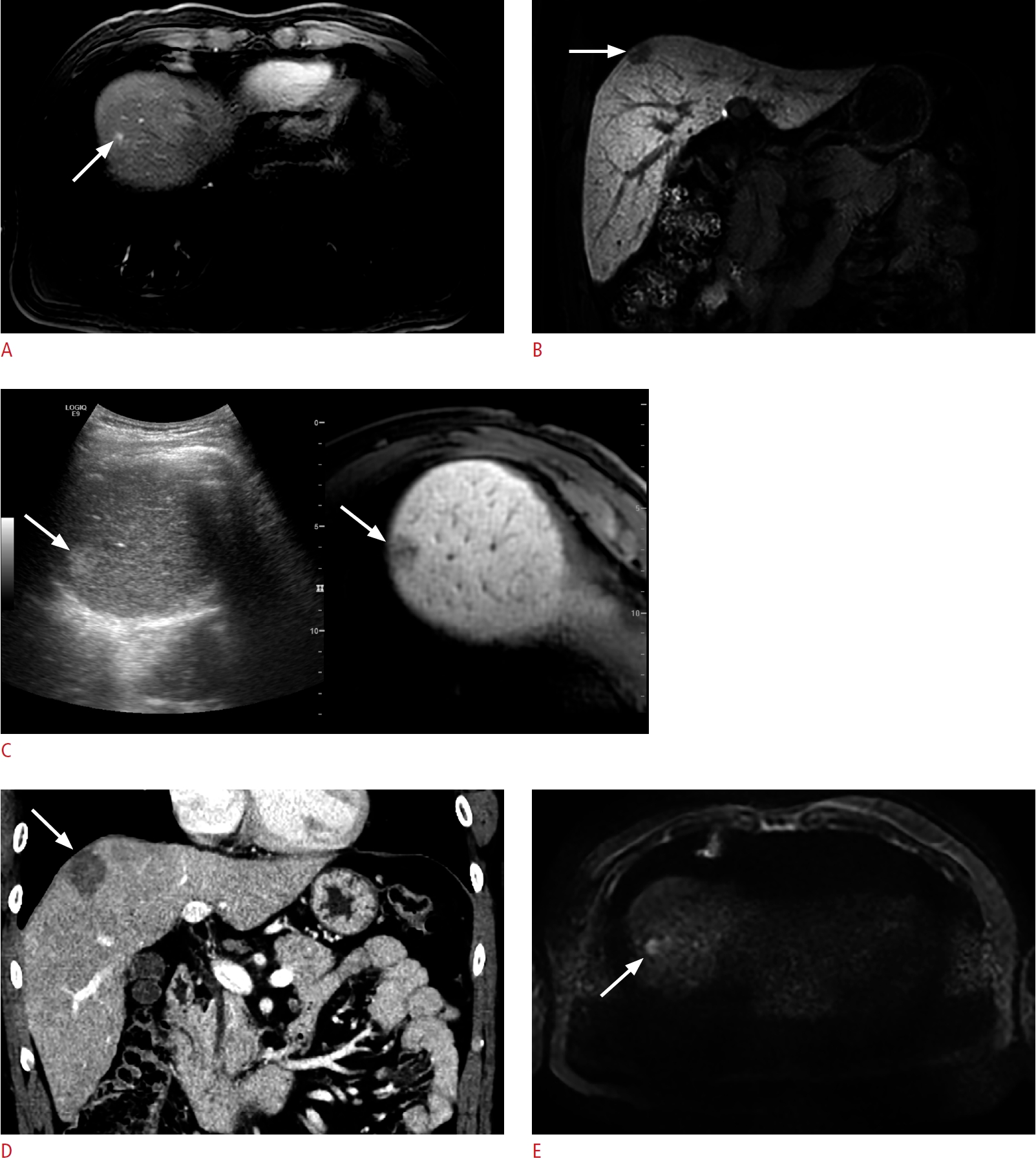
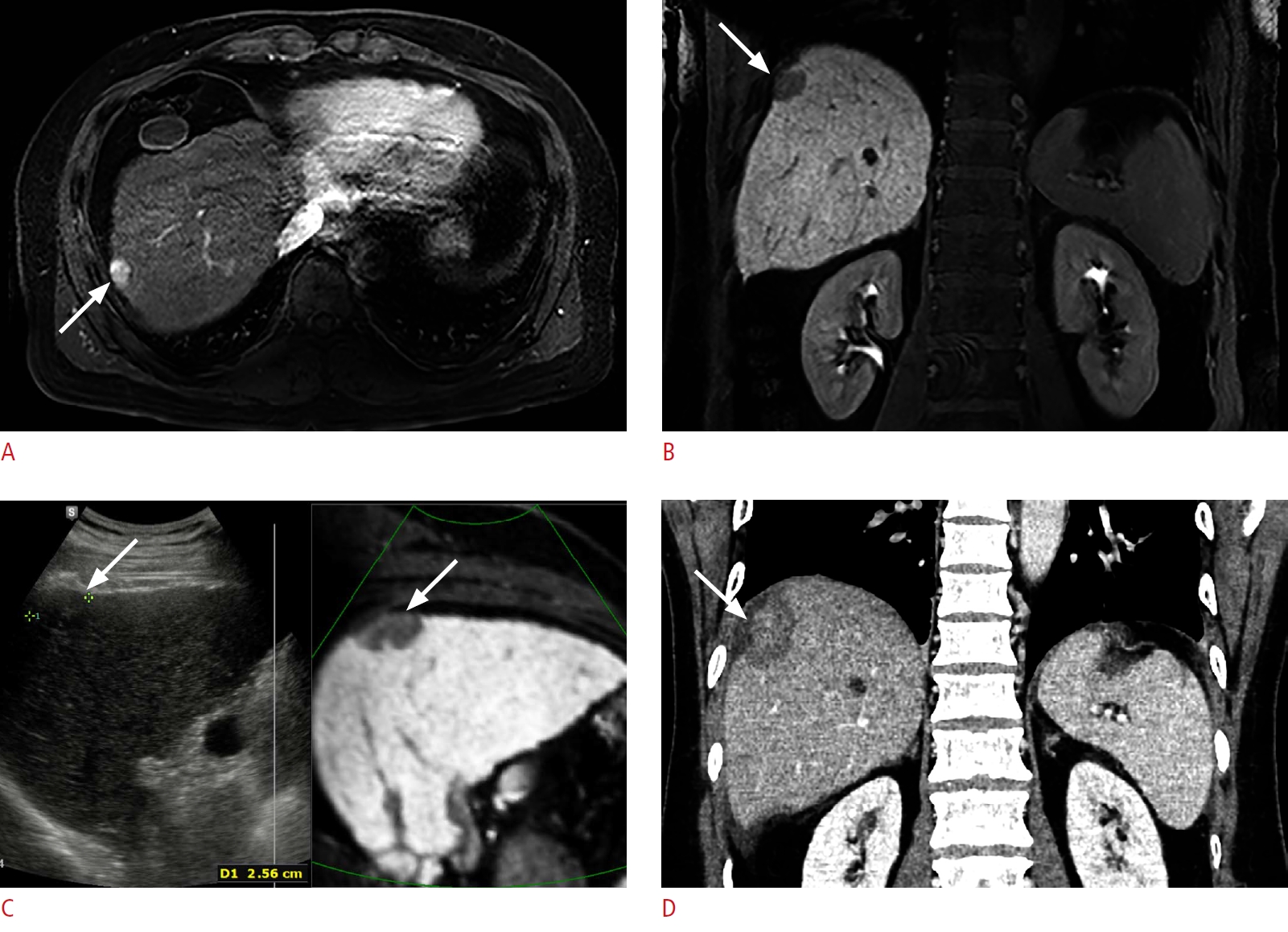
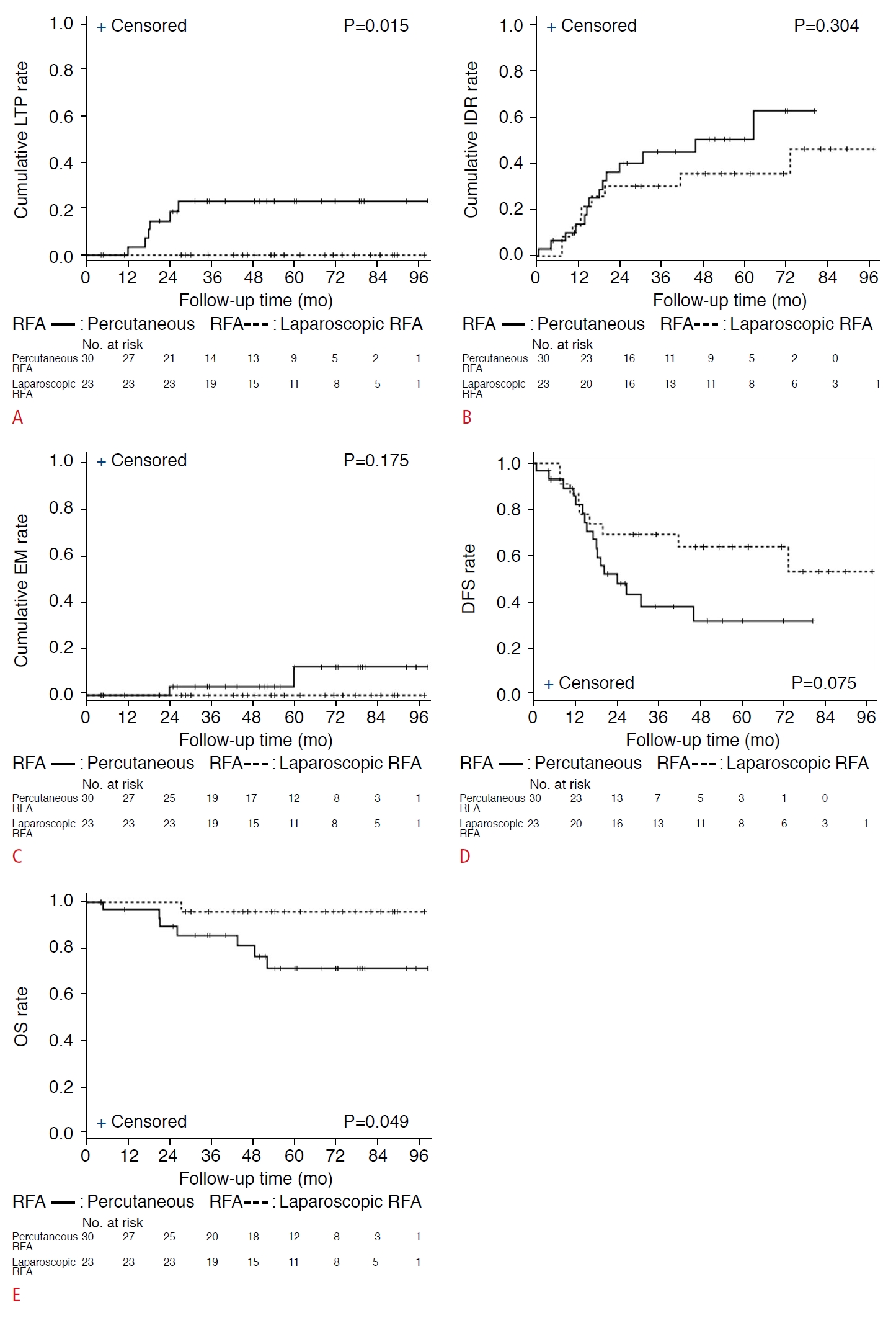
The median follow-up period was 51.9 months (range, 31.4 to 72.7 months) in the PRFA group and 57.1 months (range, 45.2 to 82.1 months) in the LRFA group. During follow-up, LTP was observed in 6 of 30 patients (20%) in the PRFA group, whereas it did not occur in the LRFA group (Figs. 2, 3). The cumulative LTP rates at 1, 3, and 5 years were estimated to be 3.7%, 23.4%, and 23.4%, respectively, in the PRFA group and 0.0% in the LRFA group (P=0.015) (Fig. 4A).
Cumulative IDR rate
IDR was observed in 14 of 30 patients (46.7%) in the PRFA group and nine of 23 patients (39.1%) in the LRFA group during follow-up. The cumulative IDR rates at 1, 3, and 5 years were 14.1%, 45.1%, and 50.6%, respectively, in the PRFA group and 13.0%, 30.4%, and 35.8%, respectively, in the LRFA group (P=0.304) (Fig. 4B).
Cumulative EM rate
EM was observed in two of 30 patients (6.7%) in the PRFA group during follow-up. Single pulmonary metastasis occurred 5 years after PRFA in one patient. Lobectomy was planned for metastasis, but the patient refused surgical treatment. In another patient, a single peritoneal seeding nodule occurred 2 years after PRFA, and surgical removal was done for the seeding nodule. IDR also developed in both patients. No EM was found in the LRFA group. The cumulative EM rates at 1, 3, and 5 years were estimated to be 0.0%, 4.0%, and 12.0%, respectively, in the PRFA group and 0.0% in the LRFA group (P=0.175) (Fig. 4C).
DFS and OS
As of April 30, 2021, seven of 30 patients (23.3%) in the PRFA group and 1 of 23 patients (4.4%) in the LRFA group died. The DFS rates at 1, 3, and 5 years were 82.2%, 38.6%, and 32.2%, respectively, in the PRFA group and 87.0%, 69.6%, and 64.2%, respectively, in the LRFA group (P=0.075) (Fig. 4D). The OS rates at 1, 3, and 5 years were 96.6%, 85.7%, and 71.6%, respectively, in the PRFA group and 100%, 95.7%, and 95.7%, respectively, in the LRFA group (P=0.049) (Fig. 4E).
Complications and Hospital Stay Duration
Major complications were found in zero (0%) patients in the PRFA group and one (4.4%) patient in the LRFA group, respectively (P=0.434). In one patient, lung and liver abscesses were found 8 months after LRFA. The patient was treated with antibiotics without external drainage.
The duration of the hospital stay was significantly different between the two groups (PRFA: median, 3 days; range, 3 to 3 days vs. LRFA: median, 5 days; range, 4 to 6 days; P<0.001).
Discussion
This study compared the treatment outcomes between LRFA and PRFA in patients with single, small (1-3 cm) subphrenic HCCs. Although LRFA required general anesthesia and a longer hospital stay than did PRFA (median, 5 vs. 3 days; P<0.001), both treatments were equally technically effective based on the 1-month follow-up CT images. The major complication rate was not significantly different between these two techniques. However, the LTP rate was significantly lower in the LRFA group than in the PRFA group. Notably, LTP was not observed in the LRFA group. The cumulative OS rate was significantly higher in the LRFA group than in the PRFA group. DFS rate was not significantly different between the two groups.
Studies directly comparing the outcomes between PRFA and LRFA for HCC are rare. LRFA has been reported to reduce the risk of multiple intrahepatic recurrences, including LTP, compared to PRFA [13]. However, more than half of a previous study population had tumors in other than subcapsular locations. In a large series [19], LTP was found in 15% of cases after LRFA, which appears to be higher than that in the present study. However, a direct comparison is difficult because the study population may be different, and only 35% of the tumors had superficial locations. As would be expected, the LTP rate was reported to be lower in subcapsular tumors [19,20]. A recent study found that invisible HCC on laparoscopy was a risk factor related to technical failure after initial LRFA attempts [14]. Therefore, subphrenic HCC visible on laparoscopy may be the best candidate for LRFA. Herein, the 5-year cumulative LTP rate significantly differed between the groups (0.0% vs. 23.4%, P=0.015). Since only subphrenic HCCs were included, excellent local tumor control after LRFA over PRFA may be expected.
Studies have examined the therapeutic outcomes after PRFA for subphrenic HCC. LTP was previously observed in 29% of subphrenic HCCs after PRFA, which was significantly higher than the 6% rate for non-subphrenic HCCs [11]. The cumulative LTP rates after PRFA were relatively high (22.5%, 37.8%, and 46.6% at 1, 3, and 5 years, respectively) [12]. These findings imply that subphrenic HCCs are challenging to control with PRFA under US guidance, even though artificial ascites is infused to enhance the sonographic window.
The difference in local tumor control between LRFA and PRFA may be attributed to the difference in technical difficulty. In PRFA, accurate electrode placement along the long trajectory under US guidance and obtaining a sufficient ablative margin along the liver surface are sometimes difficult for subphrenic tumors because the liver dome is difficult to visualize with US owing to the poor sonic window [3]. Furthermore, collateral thermal injury to the diaphragm may occur even with artificial ascites, which can lead to suboptimal ablation during PRFA. In LRFA, air is insufflated into the peritoneal cavity to provide sufficient space between the tumor and diaphragm. Therefore, it is possible to observe the liver dome directly and discriminate subphrenic tumors from the liver surface through the laparoscope. Thus, direct tumor puncture can be avoided by using multiple radiofrequency electrodes or multiple overlapping ablations. Consequently, sufficient ablative margins can be obtained after LRFA [14]. Moreover, patients’ breathing can be controlled during general anesthesia, facilitating accurate needle placement.
In the present study, after LRFA, the ablation zone was significantly larger than that of the PRFA group in comparison to the tumor. This result may be explained by the following factors. First, in general, pneumoperitoneum associated with laparoscopic procedure results in up to a 40% reduction of portal venous flow, increasing the size of the ablation zone [21-24]. Second, direct tumor puncture was avoided based on visual inspection on laparoscopy, which would have resulted in a relatively peripheral tumor puncture or even no tumor puncture in the LRFA group, thereby enabling a larger ablation zone.
Tumor location is an important factor for LTP after RFA for HCC. Subphrenic tumor location was considered a risk factor for LTP after PRFA, but a factor associated with lower LTP rates after LRFA [3,19,25]. The results of the present study confirmed that local tumor control for subphrenic HCC is more effective with LRFA than with PRFA. Thus, LRFA can be applied for subphrenic HCC if the laparoscopic approach is technically feasible.
The DFS rate was higher in the LRFA group than in the PRFA group; however, the difference was not significant. The OS rate was significantly higher in the LRFA group than in the PRFA group. These results agree with previous findings that LRFA was significantly associated with favorable OS outcomes, while DFS was not significantly different between the groups [13].
The present study had several limitations. First, this was a retrospective, single-center study. Therefore, selection bias could not be avoided. Second, the sample size was relatively small because many patients were excluded as the present study focused on a specific tumor location. Therefore, exact matching between the groups was not feasible. However, there was no significant difference in patient and tumor characteristics between the two groups. Further well-designed prospective studies are warranted to verify the results. Third, the ablative margin-a factor related to local tumor control-was not assessed in the present study, as nearby anatomic landmarks such as hepatic vessels were usually far from the tumor due to the subphrenic tumor location, making it challenging to assess the ablative margin. Fourth, there may have been bias associated with each operator’s preference, which may have influenced the choice between LRFA and PRFA.
In conclusion, LRFA showed better therapeutic outcomes in terms of LTP and OS than did PRFA for subphrenic HCC. Therefore, LRFA can be a valuable treatment option for subphrenic HCC if accessible using the laparoscopic approach.

 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



