

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Lymph node involvement is of the utmost importance in the management of patients with melanoma, as it affects their prognosis and the choice of an appropriate surgical procedure [1-3]. Since 66% of recurrent melanomas develop in the regional lymph node basin, regional lymph nodes are an important target of surveillance even after surgery [4]. In-transit metastasis, which represents non-nodal cutaneous or subcutaneous disease between the primary site and the regional lymph node basin, and distant metastasis are also important prognostic factors that influence treatment strategies [5-9]. Ultrasonography (US) has proven to be an excellent imaging modality for the initial and follow-up evaluation of metastatic lesions and provides guidance for histologic confirmation procedures in patients with melanoma [2,10-12]. Numerous studies have reported that US is superior to palpation in the detection of metastatic lesions [10,11,13]. These results suggest that US can aid in the detection and management of metastatic lesions that are nonpalpable, possibly due to their small size, deep location, or overlying fibrotic scar tissue related to previous surgery.
In patients with nodal recurrence after previous excision, excision of the recurrent lesion is recommended according to clinical practice guidelines [14]. Moreover, in patients with clinically positive lymph node metastasis identified during the initial workup, complete lymph node excision, including the identified lesion, in addition to excision of the primary tumor is recommended as the primary treatment [14]. Additionally, definitive surgical resection has been proven to be effective for in-transit or distant metastases, although they are considered to be indicators of advanced disease [8,9]. Thus, it is desirable for surgeons to easily recognize histologically confirmed or suspected metastases that are not palpable during surgery to achieve accurate removal of these lesions. Preoperative localization can be a useful option for such cases. A number of techniques for the localization of nonpalpable metastatic melanoma have been proposed, such as insertion of a wire or radioactive material within the targeted lesion under imaging guidance [15-19]. However, those procedures were reported in an extremely small number of cases and have not been established as standard treatment.
US-guided tattooing using a charcoal suspension has been widely performed for the preoperative localization of nonpalpable metastases in thyroid and breast cancer [20-25]. It has been accepted as a safe and effective procedure for indicating the location of the targeted lesions before surgical excision. To our best knowledge, no data have been reported on US-guided charcoal tattooing for the preoperative localization of nonpalpable metastatic melanoma. We hypothesized that tattooing metastatic melanoma lesions would allow them to be reliably identified intraoperatively and aid in their excision.
In this study, we evaluated the effectiveness of US-guided tattooing using a charcoal suspension for the preoperative localization of nonpalpable metastatic melanoma, mainly focusing on its visibility during surgery and the successful removal of the lesions thereafter.
Materials and Methods
Patients
Our institutional review board approved this retrospective study, and the requirement for informed patient consent was waived. From November 2009 to June 2019, we identified 29 consecutive patients with malignant melanoma (16 men and 13 women; median age, 60 years; range, 25 to 84 years) who underwent preoperative US-guided charcoal tattooing of 65 nonpalpable lesions. All patients included in the study met the following criteria for US-guided charcoal tattooing: (1) history of histologically confirmed primary malignant melanoma; (2) metastatic lesions that were either histologically confirmed or suspected based on an imaging study performed prior to US-guided charcoal tattooing; and (3) follow-up US performed within 6 months postoperatively.
US-Guided Charcoal Tattooing Procedure
A sterilized 3% w/w aqueous suspension of activated charcoal granules (Duksan Pure Chemicals, Ansan, Korea) was prepared at the Division of Pharmaceutical Services of our institution. Activated charcoal (0.3 g) was added to 10 mL of normal saline, and the suspension was filtered through a blue filter with a pore size of 0.2 ╬╝m. The preparation was distributed in 10 mL bottles and sterilized in 120┬░C steam for 20 minutes [20,21].
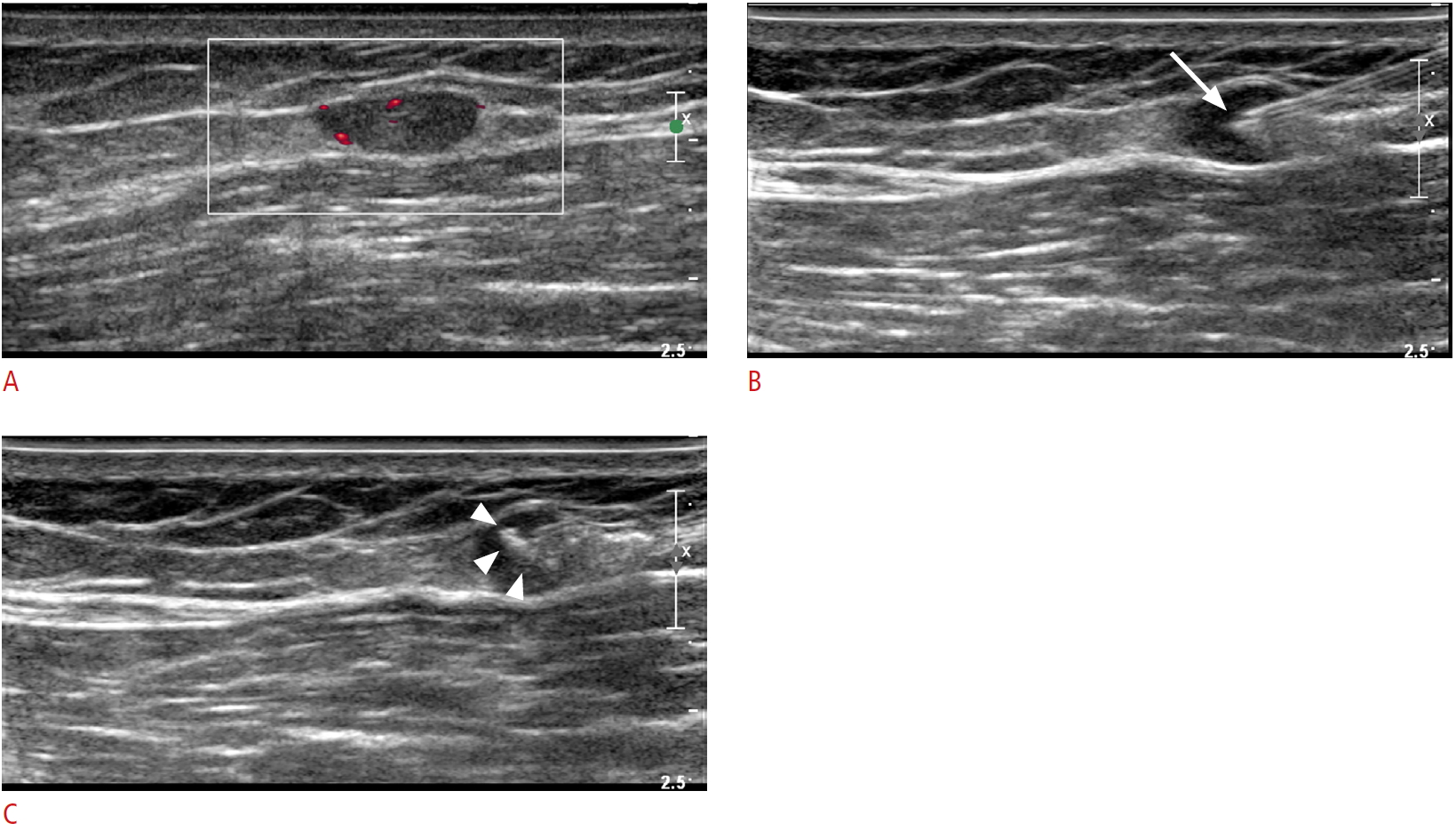
Tattooing procedures were performed by either musculoskeletal staff radiologists or musculoskeletal radiology fellows. After identifying the lesions by US, 1% lidocaine was injected into the skin selected as the entry site for local anesthesia. Then, <1 mL of the charcoal suspension was aspirated using a 5-mL syringe and an 18-G needle to prevent blockage by precipitation. A 12-5 or 15-7 MHz linear transducer (iU22, Philips Medical Systems, Bothell, WA, USA) was used for guidance and image acquisition depending on the examiner's preference. With the US transducer placed parallel to the needle to allow real-time guidance, a needle was advanced into the lesion until its tip was located at the center. The charcoal suspension was injected slowly as the needle was withdrawn to the point of skin entry (Fig. 1). Skin marking was done at the entry site to enable the surgeons to identify the site easily.
Assessment of the Effectiveness of US-Guided Charcoal Tattooing Localization
The characteristics of the patients and tattooed lesions were determined by a retrospective review of patientsŌĆÖ electronic medical records. The effectiveness of this procedure was evaluated in terms of the percentage of intraoperatively detected and removed lesions without residua on follow-up US of all tattooed lesions. US images were obtained during follow-up performed within 6 months postoperatively, and surgical and pathological reports were retrospectively reviewed. Moreover, the occurrence of procedure-related complications was analyzed.
Results
Table 1 summarizes the baseline characteristics of the 29 patients who underwent preoperative US-guided tattooing localization for histologically confirmed or suspected metastatic malignant melanoma. The lower extremity was the most common location of the primary malignant melanoma (22 of 29, 75.9%), followed by the upper extremity, trunk, and anus. A majority of the patients (22 of 29, 75.9%) underwent US-guided charcoal tattooing for recurrent disease.
The histologic characteristics of the 65 tattooed lesions in the 39 US-guided tattooing procedures are shown in Table 2. Most lesions (61 of 65, 93.8%) were initially detected by US performed prior to the tattooing procedure, while the other four lesions were initially detected by 18F-fluorodeoxyglucose-positron emission tomography/computed tomography (18F-FDG PET/CT, n=3) and contrast-enhanced computed tomography (CT, n=1). Moreover, 38 lesions (58.5%) were histologically evaluated prior to tattooing, by either US-guided fine needle aspiration (n=23) or core needle biopsy (n=15), which revealed metastases in 18 and 15 cases, respectively. In some cases, tattooing was requested by a clinician for lesions with inconclusive histology (n=2) or inadequate tissue specimen quality (n=3). Twenty-seven (41.5%) lesions that required tattooing did not undergo histological confirmation, but metastases were suspected based on the following imaging studies: 18F-FDG PET/CT alone (n=9); US alone (n=12); both PET/CT and US (n=5); and CT (n=1). Six of the lesions were benign, consisting of reactive lymph nodes (n=5) and traumatic neuroma (n=1) according to the final pathology report. Otherwise, the final pathology reports revealed that all lesions were metastases (59 of 65, 90.8%), including metastatic lymph nodes (n=51), muscle metastasis (n=5), and intransit metastasis (n=3).
The mean size of the lesions measured by US during the procedure was 9.8 mm (range, 1.3 to 24.4 mm), and the majority of them were located in the inguinal area and thigh (Table 3). There were two lesions with a diameter >2 cm that were not palpable due to their deep location within the muscle layer and overlying postoperative fibrosis with seroma. Most lesions were located in the subcutaneous fat layer (60 of 65, 92.3%). Fourteen lesions were in close proximity to a major vessel or spermatic cord. The mean time required for the procedure was 13 minutes (range, 4 to 27 minutes), and the mean time interval between tattooing and surgery was 5.4 hours (range, 1 to 24 hours).
During surgery, all but four tattooed lesions (61 of 65, 93.8%) were detected and removed by the surgeons (Fig. 2). One of the four undetected lesions was located deep in the spermatic cord. After follow-up US that revealed the remaining lesion, US-guided tattooing of the lesion was performed again, and the lesion was successfully removed by subsequent surgery. One of the other undetected lesions was located in the thigh, and two were located in the calf. The lesion in the thigh was removed by subsequent surgery after repeated US-guided tattooing; the lesions in the calf were removed with the guidance of intraoperative US. No relevant complications were noted in the medical records or radiology reports of the patients who underwent US-guided tattooing procedures.
Discussion
The management of melanoma requires a multidisciplinary approach, but surgical removal still remains the mainstay of treatment for primary tumors with regional lymph node, in-transit, or distant metastasis and locoregional recurrent disease [8,9,14,26,27]. US has been widely used for surveillance of metastatic lesions and guidance for aspiration or biopsy in patients with melanoma, but its role in the localization of nonpalpable metastasis to aid in precise surgical removal has been scarcely reported [13]. We hypothesized that US could contribute to the surgical management of patients with metastatic melanoma by guiding preoperative lesion localization with a charcoal injection.
Our results showed that US-guided tattooing localization using a charcoal suspension could effectively facilitate the subsequent surgical removal of nonpalpable metastatic melanoma. Most tattooed lesions (61 of 65, 93.8%) could be identified and removed intraoperatively. This result is comparable to the result of the US-guided tattooing performed for metastatic lesions in breast and thyroid cancer [20,23,28]. Two of the four lesions that were unsuccessfully excised after initial localization could be removed after repeated tattooing localization, while the other two lesions were removed under intraoperative US guidance. The tattooing procedure enabled the localization and removal of relatively small lesions, with a mean size of 9.8 mm, which is comparable to the size of the target lesions in previous reports on US-guided tattooing localization [20,22]. Some of the lesions were in proximity to major vascular structures, but no significant procedure-related complications were noted. According to a previous study on the US-guided tattooing localization of metastatic cervical lymph nodes in thyroid cancer, lesions adherent to the major neck vessels, such as the common carotid artery and internal jugular vein, could be safely tattooed without any complications [23].
The preoperative localization of metastatic melanoma using a wire has been reported in a few studies [16,18,19]. Those studies have suggested that wire localization can be a useful procedure to facilitate the surgical removal of nonpalpable metastatic melanoma, yet the number of studied cases was small. Presurgical wire localization has been mainly studied in nonpalpable breast lesions [29,30]. Complications related to wire insertion in breast lesions, such as wire migration, wound infection, and bleeding have been reported [31-33]. Compared to the wire localization technique, tattooing localization has a number of advantages. Since the wire is inserted from outside the patientŌĆÖs body, it can cause discomfort and pain. In contrast, the tattooing procedure causes less discomfort in the patient after the procedure, which may allow tattooing of multiple lesions. Additionally, to prevent wire migration after its placement to localize the lesion, it is essential that surgical removal of the lesion is performed as soon as possible after the procedure is completed [34]. In contrast, previous studies on preoperative tattooing localization have reported that the charcoal suspension persists for months after its injection [20,28,35]. Although it would be desirable to have a short interval between tattooing localization and surgery, the stability of the charcoal suspension may reduce scheduling issues for surgery. The localization of metastatic melanoma with intralesional injections of radioactive seeds has also been reported, but in limited cases [15,17]. Further studies with larger cohorts are needed to compare the efficacy and safety of these procedures in patients with melanoma.
We could not find any relevant complications in the medical records or radiology reports of the patients we analyzed, even though there may have been unreported minor complications. Charcoal tattooing is not considered to be a significantly demanding procedure for patients and reported to be well tolerated without severe pain, even in the head and neck region, which has rich innervation and vulnerability to pain [36,37]. Charcoal itself is an innocuous substance that has been used to localize malignant lesions over the past decades [23]. To the best of our knowledge, no major complications, including toxicity, related to charcoal have not been reported in the setting of preoperative tattooing localization for malignancies [20-25,37]. Nonetheless, it would still be desirable to have larger-scale data to ensure the long-term safety of this procedure in patients with melanoma in future studies.
Five lesions were shown to have inconclusive histology or an inadequate tissue specimen after aspiration prior to tattooing. Although aspiration cytology offers excellent diagnostic accuracy in the diagnosis of metastatic melanoma [38], an accurate diagnosis can be hindered by inadequate quality of the acquired specimen, and in such cases, surgical excision is required for a definitive diagnosis. Moreover, when multiple suspicious lymph node metastases are detected on US, a cytologic evaluation cannot be conducted for all suspected lesions. In such cases, US-guided tattooing can be used to mark those suspected lesions in addition to the cytologically proven metastasis. We believe that US-guided tattooing localization may also play a role from a diagnostic perspective in aiding surgical excision to establish accurate assessment of metastatic lesions.
Our study has several limitations. First, even though this procedure has been accepted as safe for a number of malignancies, a long-term follow-up evaluation of its potential effects on recurrence (possibly related to the procedure) in patients with melanoma has not been performed. Nonetheless, we believe that the benefit of this procedure in aiding the intraoperative detection and removal of nonpalpable lesions overwhelms this potential risk. Second, the successful surgical removal rate was not compared with that achieved using other localization methods or without localization. Third, a personŌĆÖs level of experience performing the procedure may have a certain influence on the rate of successful localization. Finally, even though the amount of injected charcoal was extremely small, it was not recorded. Likewise, the exact amount of charcoal required to optimize visibility during surgery remains to be confirmed.
Therefore, US-guided tattooing localization using a charcoal suspension can be an effective method of facilitating visual localization of nonpalpable metastatic melanoma lesions. Further studies are warranted to evaluate the long-term benefits and potential complications of the procedure and to compare its effectiveness with that of other localization methods or no localization in patients with melanoma.

 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



