

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Deep vein thrombosis (DVT) occurs when a thrombus forms in one or more deep veins. It is a common clinical problem and usually affects the lower limbs; moreover, orthopedic surgery is a known risk factor for DVT [1]. DVT can lead to pulmonary thromboembolism or post-thrombotic syndrome, which can result in death. Therefore, orthopedic surgeons usually plan to identify DVT in the lower extremities. Although it is well known that ultrasonography is an excellent modality for postoperative evaluations of orthopedic patients, and venous Doppler ultrasonography is the standard imaging modality for patients with suspected DVT, the procedure can be limited due to issues with the acoustic window and patient discomfort after surgery [2,3]. Moreover, computed tomography angiography (CTA) of the femoral vein is an alternative imaging modality, but involves potentially harmful radiation exposure, the administration of iodinated contrast agents, and a higher degree of invasiveness than ultrasonography. Therefore, it would be helpful to prioritize patients with significant risk factors who would truly benefit from postoperative ultrasonography.
The presence of DVT is associated with multiple factors. A previous study suggested that prolonged surgery (≥2 hours) and a higher body mass index were significantly associated with the development of DVT in patients undergoing major orthopedic surgery [4]. Another study reported that major orthopedic surgery was associated with a greater risk for DVT [5]. However, contradictory studies have also reported that cardiovascular disease (CVD) risk factors, such as age, smoking, adiposity, cholesterol and triglyceride levels, and diabetes mellitus (DM), were associated or not associated with venous thromboembolism [6,7]. The risk factors associated with lower-limb surgery, especially in elderly patients undergoing total knee joint replacement, and controversies regarding the prevalence of DVT, site, and host-related factors, have led to uncertainty regarding which patients require a more rigorous work-up for venous thromboembolism.
Accordingly, the objectives of the present study were to verify which patients need post-orthopedic surgery examinations for DVT by identifying the factors associated with post-orthopedic surgery DVT at our hospital and to determine whether any specific level of vessel is more vulnerable to DVT after lower-extremity surgery in order to help triage patient management in the long run.
Materials and Methods
Design, Sample Population, and Inclusion/Exclusion Criteria
This retrospective cohort study used data extracted from medical records and case information. The data remained anonymized, and no patients were directly involved in setting the research questions or the outcome measures, nor were they involved in the recruitment or implementation of the study. The requirement for informed consent was waived due to the retrospectively used medical records. It was approved by the Institutional Review Board (GDIRB 2020-330) and was conducted at Gachon University Gil Hospital (Incheon, Korea) between January 2018 and December 2019. A total of 104 potentially eligible patients, who were referred for an ultrasound work-up for suspected DVT after orthopedic surgery, and for whom the orthopedic surgeon requested ultrasonography and not computed tomography (CT) for postoperative DVT evaluation during the study period, were included. Individuals with confirmed DVT before surgery and those who underwent surgery of the upper extremities were excluded. As such, 99 patients were ultimately included in the present study.
DVT Diagnosis
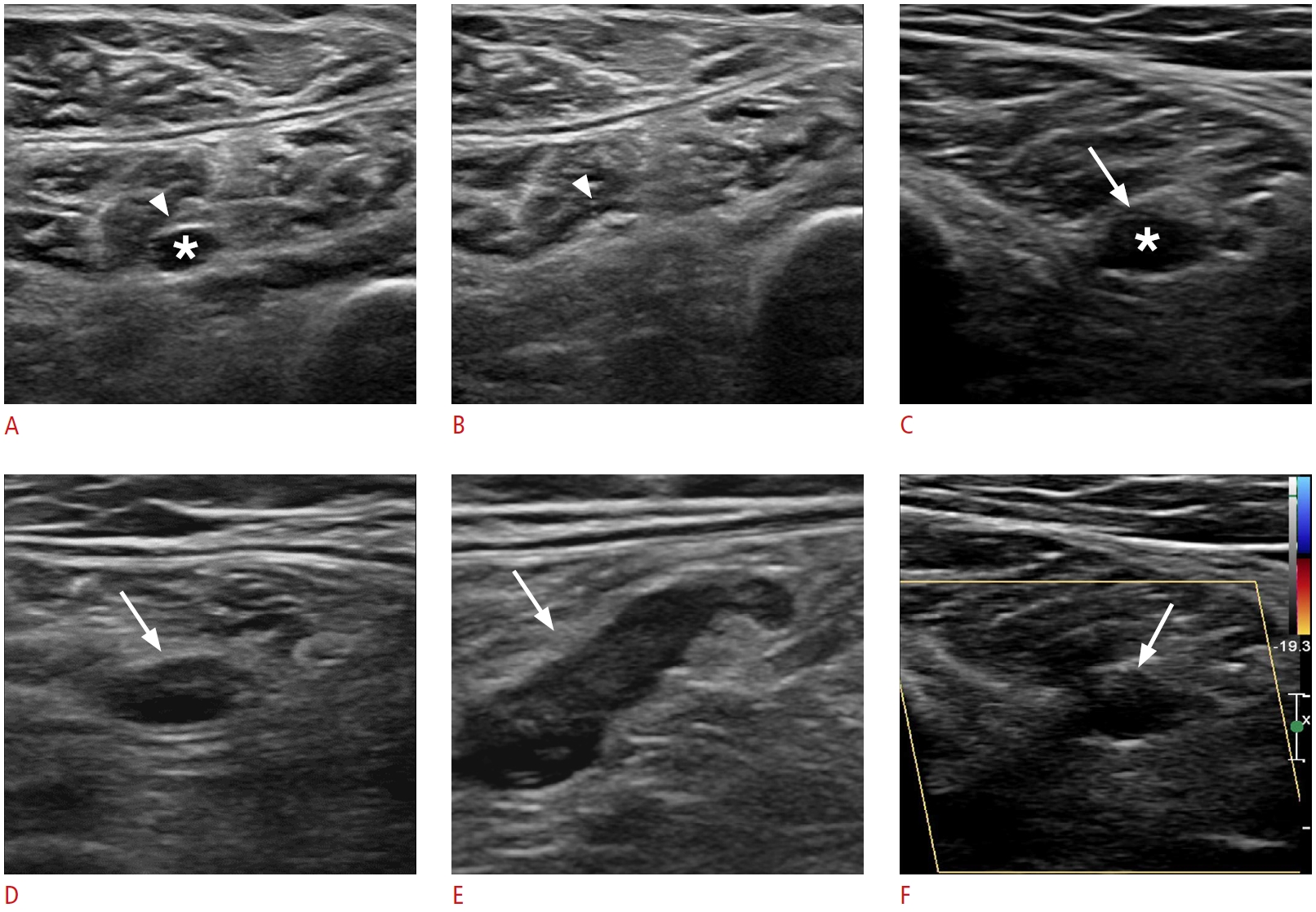
All DVT examinations were performed using a linear phased-array transducer (EPIQ 7G, Philips Healthcare, Best, Netherlands) by one of eight radiology residents under the supervision of one of four musculoskeletal radiologists. The examination followed a set protocol irrespective of the examiner’s expertise, using the two-dimensional compression technique in the supine or prone position throughout the leg, tracing the deep veins from the inguinal ligament to the femoropopliteal and tibioperoneal trunk on the transverse plane. A 3- or 5-MHz probe was applied, depending on the patient’s anatomy and the adequate depth of penetration for an optimal examination of the deep veins. Color Doppler imaging was used as a road map and only if the calf veins were inadequately visualized on real-time imaging alone. We diagnosed DVT with comprehensive duplex ultrasound combined with Doppler rather than a limited or complete compression-only examination. The mean scanning time was 10 minutes per patient. The diagnostic criteria for DVT were incompressibility of the vein with probe pressure in the affected part, and an absence of flow signal in the venous thrombosed segments (Fig. 1). This technique is routinely performed at many hospitals and can be carried out using standard ultrasound equipment and personnel. The patients were divided into a DVT group (n=33) and a non-DVT group (n=66).
Data Collection and Statistical Analysis
Data were collected on age, sex, height, body weight, duration of anesthesia, type of orthopedic surgery, and CVD risk factors. We enumerated the risk factors of CVD according to the Framingham risk score, which is a 10-year CVD risk score model that reliably predicts CVD events and mortality in the next 10 years in subjects with baseline examinations free of CVD. The predictors used in the risk model included age, sex, total cholesterol, high-density lipoprotein (HDL) cholesterol, systolic blood pressure (BP), treatment status of hypertension or diabetes, and smoking status. All data were collected from patients’ medical records and laboratory investigations. Statistical analysis of the data was done using the chi-square test, independent-sample t test, and logistic regression analysis in SPSS version 22.0 (IBM Corp., Armonk, NY, USA) for Windows (Microsoft Corporation, Redmond, WA, USA). Differences with a P-value <0.05 were considered to be statistically significant.
Results
Patient Information
The demographic characteristics of all individuals enrolled in the present study, including age, sex, height, body weight, duration of anesthesia, and operative time, are summarized in Table 1. The types of orthopedic surgery performed included total knee replacement arthroplasty (n=40), ligament reconstruction (n=14), meniscectomy (n=17), open reduction and internal fixation (n=17), incision and drainage (n=8), diagnostic arthroscopy (n=1), and others including tendon repair (n=2). Medical information regarding known CVD risk is presented in Table 2. Among 99 post-orthopedic subjects, 33 had DVT (seven with a history of surgery); the thrombosis was at the popliteal vein in only one patient, while it was below the popliteal vein in the other 32 patients. The mean age, weight, and height of the non-DVT and postoperative DVT patients was 55.1±17.9 years and 65.4±12.6 years, 70.5±15.6 kg and 61.2±8.1 kg, 163.3±11.7 cm and 157.0±7.2 cm, and 26.2 kg/m2 and 24.8 kg/m2, respectively. Total cholesterol, HDL, and systolic and diastolic BP were 70.6±87.6 mg/dL and 90.8±93.1 mg/dL, 20.7±25.9 mg/dL and 26.0±26.8 mg/dL, and 133.6/80.2±15.7/9.9 mmHg, and 132.2/78.1±13.9/8.6 mm Hg, respectively. The mean duration of anesthesia was 158.9±60.9 minutes and 173.2±75.3 minutes, and the operative time was 122.7±56.1 minutes and 135.5±72.1 minutes, respectively. All patients with DVT received intermittent pneumatic compression and were initially managed with apixaban or rivaroxaban. The patients were discharged with short-term follow-up at the outpatient clinic.
Univariate and Multivariate Analyses of Risk Factors
Univariate logistic regression analysis indicated that two variables were significantly associated with the development of DVT: older age (P<0.05) and lower body weight (P<0.05). In contrast, total cholesterol, HDL, systolic and diastolic BP, mean duration of anesthesia, and operative time were not significantly correlated with postoperative DVT, although there was a rising trend in the incidence of DVT with increasing values in each category. Multivariate logistic regression also revealed the same result with regard to age and body weight (P<0.05). The risk of DVT associated with surgery increased with age and decreased with body weight (odds ratio [OR], 3.3 if >60 years; 95% confidence interval [CI], 1.3 to 8.5; OR, 3.1 if <60 kg; 95% CI, 1.3 to 7.3; P<0.05).
Discussion
Orthopedic surgery is a well-known risk factor for DVT. The release of thromboplastin from dissected soft tissue and reamed bone, as well as venous stasis during surgery and postoperative immobility, contribute to high rates of DVT [8]. The frequency of all major lower-limb orthopedic surgical procedures has increased annually, similar to what has been reported in previous studies [5]. This study investigated the incidence and causes of postoperative DVT, which has multifactorial risk factors. We found that approximately a third of postoperative patients had DVT distal to the knee, and DVT was significantly associated with older age and lower body weight.
Ultrasonography plays a role as an important imaging modality in the accurate diagnosis of postoperative DVT. Most of all, this imaging modality is not affected by metal artifacts, which is especially relevant after musculoskeletal surgery. The susceptibility of magnetic resonance imaging to artifacts, as well as the presence of streak artifacts in CT, can reduce the diagnostic performance of these modalities for DVT. Second, the flexibility of ultrasound examinations in a variety of locations and patients positions is a strength in the postoperative setting. Ultrasonography at various angles may also help overcome the poor sonic window. Third, ultrasonography is a fast, reliable, and cost-effective technique compared to other modalities. Moreover, it can be used to evaluate postoperative pathologic conditions, such as abscesses, muscles or tendon tears, or the extent of hemarthrosis [2].
A previous report showed that knee surgery had a higher incidence of DVT at the localized popliteal location [9]. Unlike the previous study, most DVT sites in our cases were distal to the popliteal vein, including the tibial, peroneal, soleus, (Fig. 2) and gastrocnemius veins; only one DVT was found at the level of the popliteal vein, and no patients had distant thromboembolism. Calf vein thromboses have been reported to be closely related with lack of limb movement. More specifically, the soleal intramuscular veins depend on muscle contraction for venous perfusion, and their valve system does not function sufficiently in immobile patients, so that these veins are the leading points of DVT in the leg. Therefore, postoperative patients, especially after lower-limb surgery, are susceptible to venous stasis due to lack of motion. Our data showed the typical location of DVTs in this context. In contrast, iliac or femoral vein lesions are mainly caused by iliac vein compression, or catheter-related injury, and are symptomatic.
The major threat of a soleal thrombus is that it can propagate silently to the thigh, and form a freely floating distant thromboembolism to the lung. Therefore, it is important to remain vigilant for calf lesions, especially in patients with a known risk for DVT [10-12].
The risk factors known to be related with DVT were analyzed in our study, and interestingly, instead of the usual suspects (e.g., prolonged surgery time or cardiovascular risk factors), we found that lower body weight was associated with a higher incidence of postoperative DVT. In one study, the relative muscle volume of the vastus lateralis at the level of the thigh was negatively associated with the prevalence of symptomatic and radiologically detected DVT [13]. Lower body weight can be accompanied by loss of muscle volume, which is known as sarcopenia. Sarcopenia is defined as the loss of skeletal muscle mass and strength with aging, and is a recognized component of geriatric syndrome [14]. It has been associated with a multitude of poor outcomes including low survival rate, high infection rate, prolonged hospital stay, treatment toxicity, and physical disability [15]. Although obesity is a known risk factor for DVT, it is uncertain whether only a higher body weight is an independent risk factor for DVT, or whether the effect is secondary to DM and dyslipidemia [16]. We suggest future research on sarcopenia, especially in the leg, which may be related to the occurrence of DVT.
In addition, low muscle mass has also negative correlations with an increased prevalence of coronary arterial disorder(s) and metabolic syndrome [17]. Future studies investigating the associations of DVT with the Framingham risk score and leg muscle mass are warranted.
The management of below-knee DVT remains inconsistent because current guidelines are based on weak evidence. The American College of Chest Physicians recommends anticoagulation if symptoms are severe; otherwise, it is recommended to perform surveillance ultrasonography 2 weeks after surgery to monitor for clot propagation, at which point anticoagulation should be initiated if there is any evidence of proximal extension [18]. Patient symptoms and a D-dimer test in the early postoperative period, however, may lead to clinical confusion and mask the thrombosis. Therefore, it is the responsibility of radiologists to clearly report sonographic findings in a way that most appropriately facilitates patient management, and recommend an alternative study such as CTA in cases of severe postoperative changes in overlying soft tissue shadowing the deep venous structure. When postoperative ultrasonography for DVT showed the presence of a thrombosis, the clinicians at our hospital treated the respective patients with antithrombotic agents, even for isolated calf vein lesions, closely monitored them at the outpatient clinic, and followed up with ultrasonography. Most DVT sites in our patients were distal to the popliteal vein, with multiple sites, including the tibial vein in five patients, the peroneal vein in 13 patients, the soleal vein in 28 patients, and the gastrocnemius veins in 25 patients. None of them had adverse events related with anticoagulation therapy or distant thromboembolism. All showed resolution of the thrombosis on follow-up. We believe that early sonographic recognition and treatment may have prevented thrombotic extension or recurrence, although this possibility needs future study.
Several limitations of this study should be acknowledged. First, data analysis was performed retrospectively at a single tertiary referral center, and some asymptomatic patients may have missed the postoperative evaluation. Second, DVT ultrasonography is considered to be an operator-dependent imaging procedure. The variable expertise of the operators may have affected the reported incidence of DVT. To decrease inter-operator variability, the study was performed using a standardized protocol, and the expert musculoskeletal radiologists confirmed the examinations. Additionally, with more expert examinations, the incidence of distal DVT might even increase, since it is more difficult to diagnose a thrombosis in a calf vein than at the femoropopliteal level in postoperative patients [19]. Third, DVT prophylaxis regimens and prevention programs may have affected the outcomes of our study.
In conclusion, isolated distal DVTs were found to be common in patients after lower-limb surgery. We showed that advanced age and lower body weight were associated with a higher incidence of postoperative DVT. The typical location was below the popliteal vein, which may be related to venous stasis. Therefore, physicians should carefully examine the calf level, especially in elderly and fragile patients. In the aging society, where more and more elderly patients with DVT risk factors undergo major surgery, we hope that the typical ultrasonography findings shown in our study will help radiologists screen at-risk patients.

 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



