

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Peliosis hepatis (PH) is a rare benign disease, which is histologically characterized by blood-filled cystic cavities of various sizes and irregular shapes. These cavities communicate with the hepatic sinusoids and are associated with rupture of the reticulin framework [1]. PH has been described as typically involving the entire liver [2], and with the progress of modern medical imaging technologies, PH is now more frequently encountered in clinical practice [3].
PH is often asymptomatic; however, it may be associated with rare, but severe complications, which include hepatic failure, portal hypertension, and liver rupture leading to hemoperitoneum and hemodynamic instability [2]. In clinical practice, an accurate preoperative diagnosis of PH can have an impact on the immediate management of patients and help avoid unnecessary surgery or biopsy, thereby reducing morbidity. Withdrawal of the causative toxin or introduction of specific treatment (such as antibiotics in bacillary peliosis [4], particularly in immunocompromised patients), can resolve the disease and prevent serious complications such as hepatic failure or death owing to intra-abdominal hemorrhage [5].
Most cases of PH are detected incidentally and have no symptoms. The imaging findings of PH are often nonspecific and vary depending on the different pathological patterns of the disease and presence of hepatic steatosis. The characteristics of PH on abdominal ultrasonography, computed tomography (CT), magnetic resonance imaging (MRI), angiography, and fludeoxyglucose positron emission tomography/CT have only been sporadically described in case reports [6,7]. The nonspecific imaging characteristics of PH have a broad spectrum and are often misleading [8]. Typically, it is difficult to clearly distinguish PH from other hypervascular lesions on imaging studies alone [1], and a histopathological evaluation is thus necessary. There is, however, an increased risk of bleeding with needle biopsy of vascular lesions [9] and therefore, the understanding of the imaging features of PH may be helpful for establishing the correct diagnosis, occasionally without the need for sampling.
According to the current European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) and World Federation of Societies for Ultrasound in Medicine and Biology (WFUMB) guidelines, contrast-enhanced ultrasonography (CEUS) as a noninvasive imaging method allows differentiation between most benign and malignant focal liver lesions [10,11]. Only a few case reports have described the incidental findings [12] and CEUS features of focal PH. To the best of our knowledge, in this study, we report the largest series to date [13]. Our aim was to investigate the ultrasound and CEUS features of histopathologically proven focal PH.
Materials and Methods
Compliance with Ethical Standards
The institutional review board of Zhongshan Hospital approved this retrospective study (ID: B2020-309R). Informed consent was waived before ultrasound examination. The procedure followed was in accordance with the Declaration of Helsinki.
Patients
Between January 2012 and May 2020, a multicenter retrospective study was performed among five institutions. Twenty-four patients with histopathologically confirmed PH (11 men, 13 women; mean age, 32.4±7.1 years; range, 28 to 41 years) were analyzed (Table 1). All lesions were histologically proven, either by 18- or 20-gauge core needle biopsy (n=10) or by hepatic surgery (n=14). All patients were examined with CEUS 2-3 days before ultrasound-guided core needle biopsy or liver resection. No exclusion criteria were defined.
Ultrasound Examination Technique
Conventional B-mode ultrasonography (BMUS) and CEUS were performed in all patients by sonologists with more than 10 years of liver CEUS experience. All ultrasound examinations were performed using one of four premium ultrasound systems: Acuson Sequoia (5C1 convex array probes, 3.5 MHz, n=3, Siemens Healthineers, Mountain View, CA, USA), S2000 HELX OXANA (6C1 convex array probes, 3.5 MHz, n=8, Siemens Medical Solution USA Inc., Mountain View, CA, USA), Philips EPIQ7 (C2-9 convex array probes, 2-9 MHz, n=6, Philips, Bothell, WA, USA), LOGIQ E9 (C1-5 convex array probes, 1-5 MHz, n=7, GE Healthcare, Milwaukee, WI, USA).
SonoVue (sulfur hexafluoride, Bracco, Milan, Italy) was used with doses ranging between 1.5 and 2.4 mL depending on patient size and local practice. It was injected intravenously through a cannula placed in the antecubital fossa vein and immediately flushed with 5 mL of normal saline solution. Still images and videoclips, recorded for up to 3 minutes after contrast agent injection, were stored for analysis.
Imaging Analysis
Two independent radiologists (with extensive CEUS experience of more than 10 years), who were blinded to the clinical and pathological data, reviewed all the stored anonymized ultrasound examinations. All CEUS features were interpreted according to the current WFUMB-EFSUMB guidelines [10,11].
The reviewers documented the following BMUS features: maximum diameter of the focal liver lesion, echogenicity (homogeneous or heterogeneous; hyperechoic, hypoechoic, or isoechoic), shape (regular or irregular), margin (well or ill-defined), presence of color flow signal. The CEUS imaging review focused on the contrast enhancement pattern of lesion (hypo-enhanced, hyper-enhanced, iso-enhanced, heterogeneous, and homogeneous) during the arterial (10-45 seconds), portal venous (30-120 seconds), and late (>120 seconds) phases of CEUS [10,11].
Histopathological Diagnosis
Seven pathologists with hepatobiliary expertise reviewed all pathological slides. The final histopathological diagnosis was based on hematoxylin and eosin-stained sections and immunohistochemical staining results.
Statistical Analysis
Statistical analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). The chi-square test and Fisher exact test were used to compare categorical parameters between two groups. Continuous parameters were presented as the mean±standard deviation, and the Student t test was used. A P-value of less than 0.05 was considered to indicate statistical significance.
Results
Clinical Findings
The indications for imaging studies in patients were regular postoperative surveillance in five patients, preoperative staging of gastrointestinal cancer in three patients, screening for hepatocellular carcinoma (HCC) in four chronic hepatitis B patients, and regular health examinations for 12 patients. Serologic tumor markers including alpha-fetoprotein, carbohydrate antigen 19-9, and carcinoembryonic antigen were all within normal ranges. Peliosis was observed in three patients with concomitant hepatocellular adenoma, in two patients with HCC, and in 19 patients without a synchronous focal liver lesion.
BMUS Features
Single lesions were detected in 17 patients, while there were multiple lesions in seven patients. Most of the lesions (83.3%, 20/24) were heterogeneously hypoechoic on BMUS, with well-defined margins but irregular shapes. No mass effect was evident in this group. Two lesions showed mixed echogenicity, but were predominantly hypoechoic. The mean size of all PH lesions was 36.8±12.4 mm (range, 10 to 80 mm) and color Doppler flow signals were detected in 41.7% (10/24) of lesions. Calculations of the spectral Doppler trace showed a mean intra-lesional resistive index of 0.45±0.13.
CEUS Features
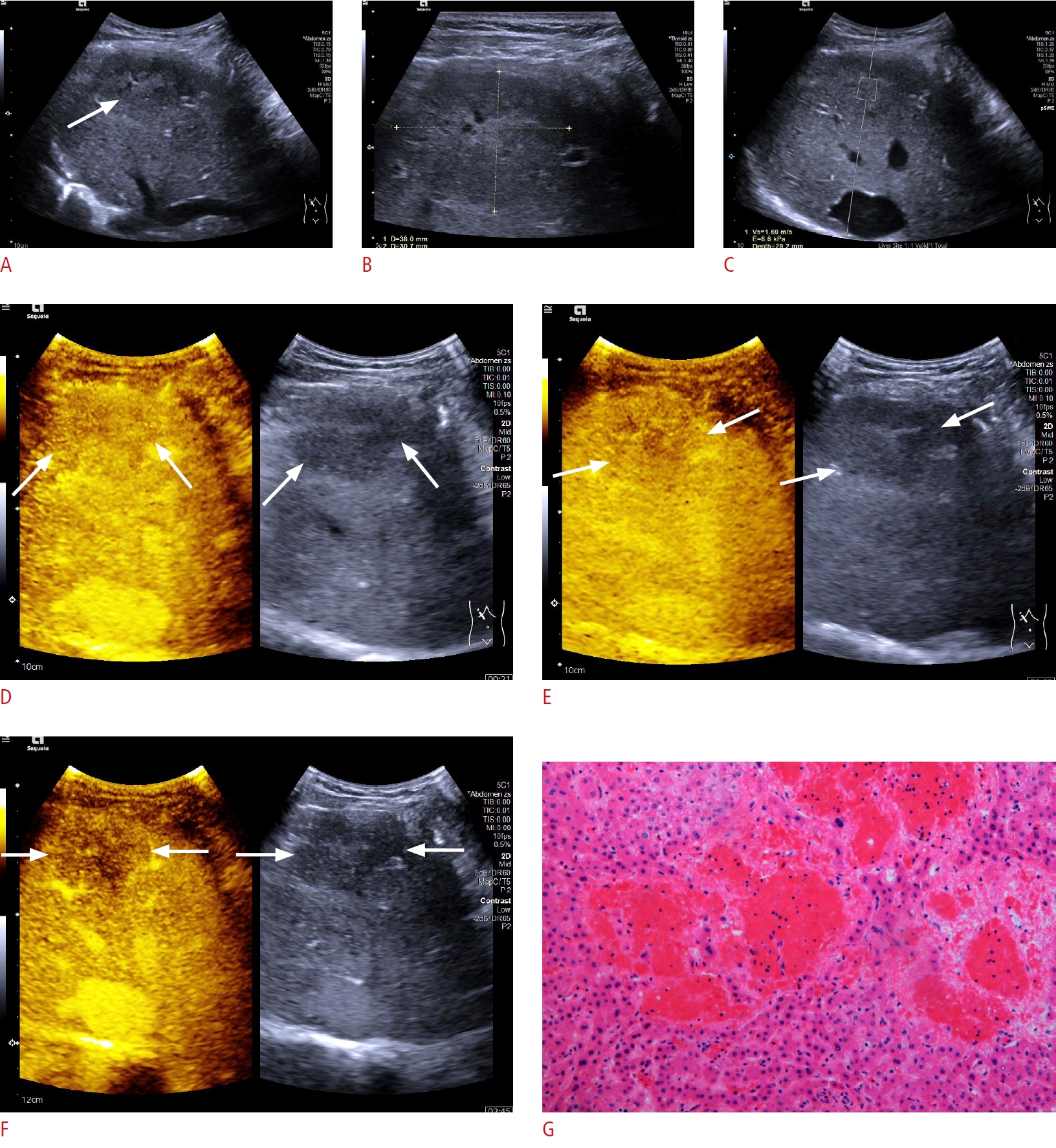
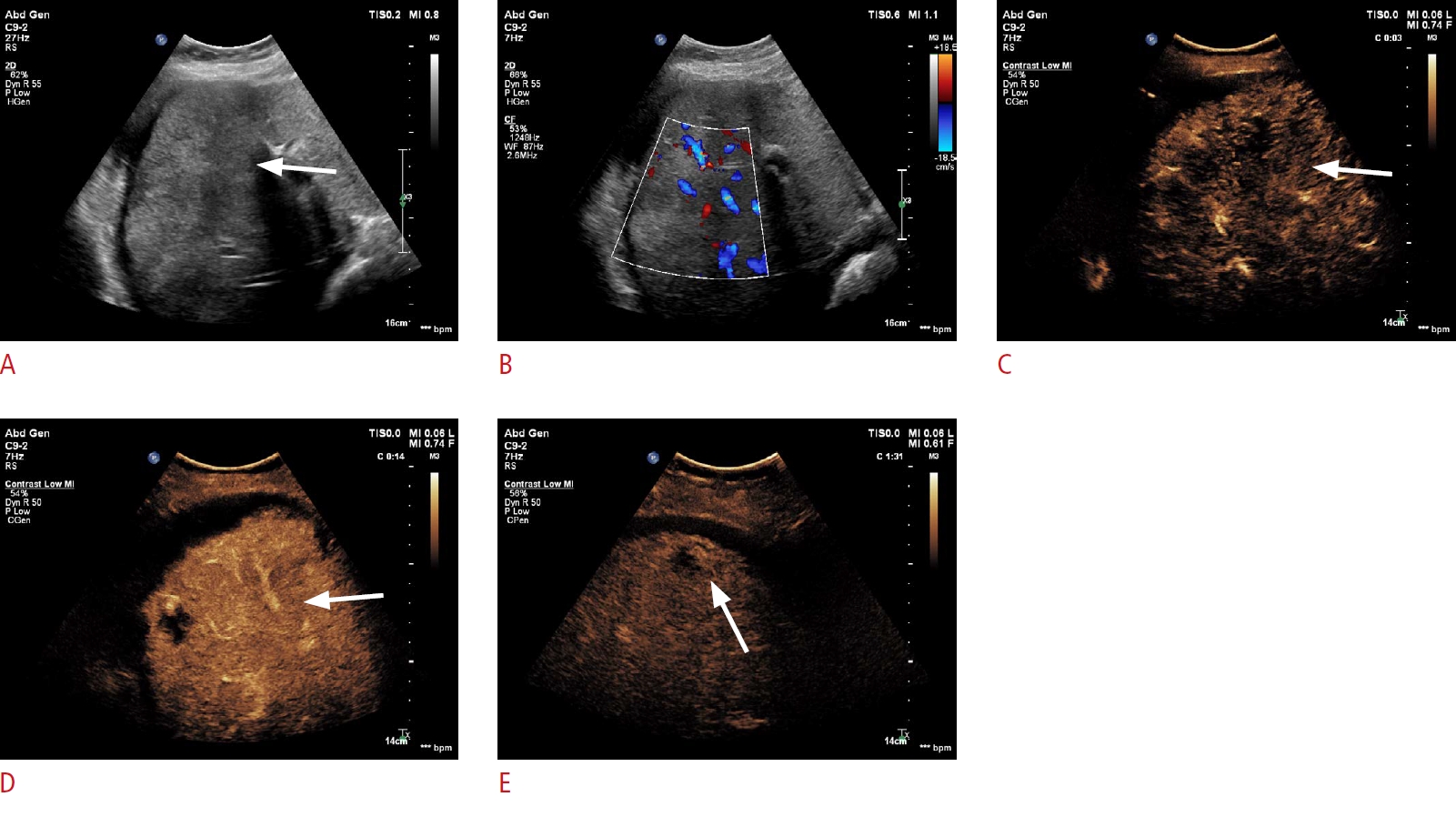
CEUS was performed in all 24 patients diagnosed with PH. During the arterial phase, the lesions displayed either mild heterogeneous hyperenhancement (83.3%, 20/24) or isoenhancement (16.7%, 4/24) compared to the surrounding liver parenchyma (Figs. 1, 2). In three cases, there was a progressive centrifugal enhancement pattern (Table 2). After 1 minute, in the portal venous phase, 21 lesions became mildly hypo-enhanced and washed out in the late phase. In our series there were three patients with phlebetactic PH who showed a strongly enhancing area in the central portion at the arterial phase, which then spread to the periphery in the progressively centrifugal direction during the portal venous and late phases (Fig. 3).
Final Diagnosis
Histopathological examinations with hematoxylin and eosin staining of the specimens revealed typical features of parenchymal PH in 21 patients, including the presence of localized irregular dilatation of sinusoids forming blood-filled spaces in the liver parenchyma, and thinning of hepatic cell cords and the reticulin fiber network. The presence of neoplastic cells was excluded (Figs. 1, 2).
In three patients with phlebetactic PH, the presence of endothelial lining along the blood-filled spaces caused by aneurysmal dilatation of the central vein was observed.
Discussion
In this study, we analyzed the imaging features of histologically-proven PH. Wagner first described PH in 1861. In 1916, Schoenlack termed it "peliosis," from the Greek word pelios, which means "livid" (i.e., discolored by extravasated blood) [14]. PH is a benign vascular condition with proliferating liver sinusoids resulting in cystic blood-filled cavities. These cysts communicate with the hepatic sinusoids and are associated with rupture of the reticulin framework [15]. The pathogenesis and etiology of PH remains unclear and is often unidentified in 20%-50% of patients [2]. It has been reported to be associated with chronic debilitating conditions (e.g., amyloidosis, chronic kidney diseases, infections, and immunocompromised status) and various drugs (e.g. steroids, oral contraceptives, and tamoxifen) [16]. In our results, there was no meaningful difference in the distribution of PH patients by sex. PH may be circumscribed or form part of a focal liver lesion, but it can also present as a widespread, diffuse feature throughout the whole liver [17]. As we show in Table 1, most of the PH lesions in this series were single lesions, while seven presented as multiple lesions in the liver. The same process may occur in the spleen, bone marrow, lymph nodes, and more rarely in lungs, stomach, intestine, parathyroid, pancreas, pituitary gland, and kidneys [14,16]. The clinical presentation of PH may range from asymptomatic to progressive cholestasis, hepatic failure, and potentially spontaneous rupture that may be fatal [2,6]. In our current study, only five patients had a history of chronic liver disease.
The imaging findings of focal PH may vary depending on the size, pathological presentation, and stage of the lesion [6]. It has nonspecific features on conventional abdominal ultrasound and can present as a homogeneous, hypoechoic lesion in patients with fatty liver, a hyperechoic lesion in patients with a normal liver, or a heterogeneous lesion if complicated by hemorrhage [7]. Previous reports have described that the imaging features of focal PH can mimic a mass and may be difficult to distinguish from other hepatic lesions including hemangioma, HCC, metastases, adenoma, focal nodular hyperplasia (FNH), and multiple abscesses [6,7,18,19]. Most cases of PH are detected incidentally as a hypervascular tumor on cross-sectional imaging (CT/MRI, ultrasonography). PH may part of the histological features of hepatocellular adenoma [8,20], HCC [21], sarcoma, FNH [20], hemangioma [8], and other focal liver lesions including focal tuberculosis, as well as severe hepatic infections [19].
In this study, primary lesions did not exhibit a marked mass effect due to their diffuse characteristics, and most appeared as hypoechoic focal liver lesions (80.9%). This is thought to correspond to the venous lakes that are commonly described histologically [7]. Two lesions were of mixed echogenicity, but predominantly hypoechoic; this may be due to the cystic cavities, thrombosis, or hemorrhage inside the vascular cavities of these lesions [7,14]. On color Doppler, it is possible to detect intra-lesional flow with typical low resistive indices on spectral Doppler [22]. Focal PH should be suspected when an incidentally detected focal liver lesion shows no specific ultrasound findings that clearly favor the diagnosis of a common tumor-like hepatic lesion [23]. The lack of a mass effect would be an even more strongly supportive finding.
The most common CEUS enhancement pattern described in our cases was mild heterogeneous hyperenhancement in the arterial phase, with washout as the most important CEUS feature in the late portal venous phase and late phase. These CEUS features of washout in the later phases are suggestive of the presence of non-hepatic tissue and thus warrant a further diagnostic work-up including a biopsy. It must be taken into account that hypoenhancement in the late phase is very rarely observed in CEUS examinations of benign focal liver lesions [10,11].
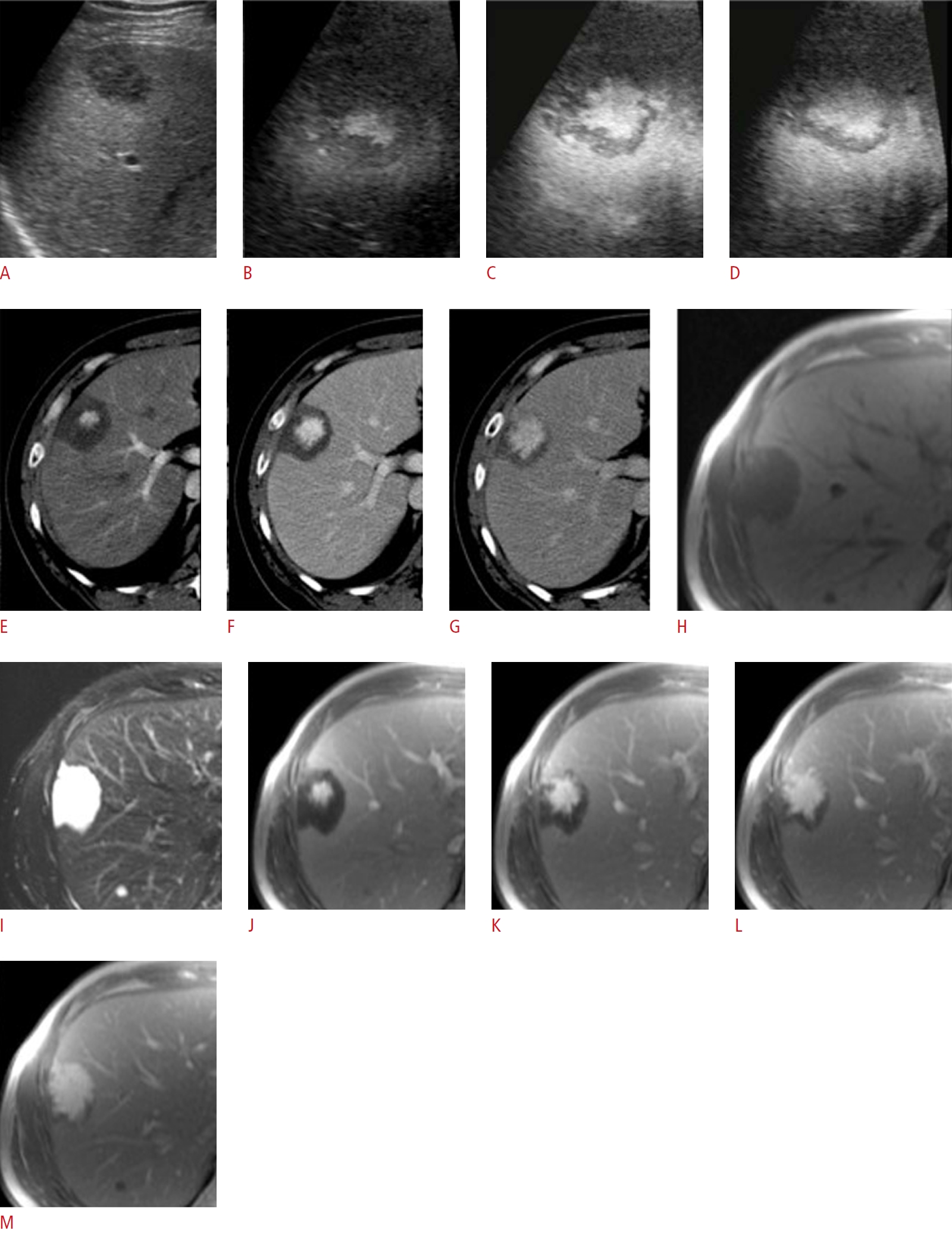
The dynamic CEUS enhancement patterns of focal PH may also vary depending on the underlying disease and the various stages of the blood components [6]. Dynamic CEUS may thus show hypoenhancement of the lesion in the late portal venous phase and late phase [24]. A similar CEUS enhancement pattern was reported in a previous case report. In contrast, "atypical" enhancement patterns, such as a peripheral ring enhancement in the arterial phase with centripetal filling and homogeneous hyperenhancement in the late phase, have been described by Gronlykke et al. [25], while peripheral hyperenhancement with central but not peripheral washout in the late phase was described by Schuldes and Weickert [26]. Central enhancement probably reflects a similar pattern of blood flow reported on CT by Gouya et al. [27], which might be a potential differentiating feature from hepatic hemangiomas. Yanoff and Rawson [28] described two types of PH (parenchymal and phlebectatic), but imaging findings of the latter type have rarely been reported [27,29]. In addition, multilocular PH may be observed (Fig. 2).
In our series, there were three patients with phlebetactic PH. The dynamic CEUS imaging features of these lesions showed a pathognomonic enhancement pattern with progressive centrifugal enhancement from the arterial into the late phase (Fig. 3). Pathologically, the main distinguishing feature of the phlebectatic PH subtype from the thrombotic PH subtype is the presence of endothelial lining along the blood-filled spaces, since it is known to be based on aneurysmal dilatation of the central vein [27,29]. This difference in blood supply is helpful to understand the hemodynamics and the "reversed" enhancement pattern of PH from hepatic hemangioma, which allows a clear differentiation between these two entities. The lack of any nodular peripheral hyperenhancement in the arterial phase of CEUS, as observed in our cases, would also be atypical for a hemangioma [5].
The imaging findings of PH in our study are somewhat similar to those described in hepatic tumors of various etiologies [6]. Thus, PH should always be considered in the differential diagnosis of focal liver lesions. The size of PH lesions ranges from a few millimeters to more than 4 cm [24], and PH appears to be a continuous process from diffuse infiltration to predominant focal infiltration. The hypoechoic images on BMUS, together with early arterial phase hyperenhancement on CEUS, may mimic HCC or liver metastasis [6]. However, the absence of a mass effect would be more suggestive of PH since peliosis presumably starts as a diffuse process. In addition, HCCs are usually hyper-enhanced in the arterial phase with relatively rapid washout in the portal venous phase compared to PH. HCC is more common in the background of chronic hepatitis or liver cirrhosis. The enhancement features of HCC have been summarized by the Liver Imaging Reporting and Data System working group [30].
Although benign, asymptomatic, and usually an incidental finding, PH should always be kept in mind as a differential diagnosis of an atypical hypervascular hepatic lesion. The other differential diagnoses would include hepatic adenomas, FNH, Caroli disease, and multiple abscesses [7,9,24], although these may have individually distinguishing features. For example, when compared to FNH, most PH lesions demonstrated heterogeneous hyperenhancement during the arterial phase of CEUS, rather than the typical avid homogeneous centrifugal pattern seen with FNH. All PH lesions also demonstrated hypoenhancement during the portal venous and late phases, while all FNH lesions typically show hyperenhancement or isoenhancement. By observing these typical CEUS features, it is possible to differentiate PH from FNH.
According to current guidelines, all focal liver lesions with washout on CEUS require a biopsy or excision for histological confirmation if not contraindicated [10,11]. Thus, a percutaneous biopsy is often necessary to reach a definitive diagnosis when PH is suspected on imaging studies [2] unless it is of the phlebetactic subtype, which has a pathognomonic CEUS enhancement pattern.
There are some limitations of our study. Owing to the rarity of this disease, the predominant limitation is the small sample size. However, to the best of our knowledge, this is the largest series of PH described in the literature. Further large-scale research will be needed to validate the ultrasound features described herein. In addition, as this was a retrospective study, various ultrasound scanners and transducers were utilized and only patients with histologically-confirmed PH were included.
In conclusion, the CEUS characteristics of focal PH are typically the lack of a mass effect on BMUS, and mild heterogeneous arterial hyperenhancement and washout in the portal venous and late phases. In the absence of malignancy, PH should be considered, particularly if the imaging characteristics are not specific for a known common hepatic lesion.
 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



