

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Trauma is the leading cause of death in people under 45 years of age [1]. Traumatic hemorrhagic shock has a high incidence and is the cause of 80% of deaths among patients with survivable trauma [1,2]. Therefore, detecting hemorrhagic shock early is critical for effectively treating trauma patients and reducing the costs of care and patient deaths [1].
Several invasive and non-invasive methods have been proposed for measuring intravascular volume and fluid loss [3,4]. Various clinical examinations, including the systolic blood pressure (SBP), pulse rate (PR), and shock index (SI), all of which have variable sensitivities, have been used for these purposes [5]. Although laboratory methods, such as evaluating blood lactate levels and the blood base deficit, have good diagnostic accuracy, they are usually time-consuming and some of these methods lack reliability. Therefore, diagnosing a hypovolemic condition-especially in the early stages of hemorrhagic shock-and occult bleeding based on clinical examinations, vital signs, and laboratory tests can be challenging [6,7].
Ultrasonography is a non-invasive, rapid, accessible, and usable clinical procedure that can be used to diagnose bleeding. Various ultrasound indices, including the inferior vena cava (IVC) diameter [8,9], IVC collapsibility index [10], IVC to aortic diameter ratio [11], and jugular index [12], have been applied to evaluate fluid loss. These methods assess vein diameter, especially the diameter of the IVC. However, the results of these methods are contradictory [9,13-15]. Moreover, IVC ultrasonography can be difficult for most trauma patients due to the abdominal fat percentage, abdominal gas, and the long time it takes to measure this parameter. It is easier to assess the internal jugular vein (IJV) than the IVC. In this regard, respiratory changes in the IJV are helpful for evaluating intravascular fluid status [7,16].
Intravascular volume loss is an inevitable consequence of bleeding. The two main parameters that affect volume loss are intravenous volume and cardiac output. These two parameters affect the flow pattern of IJV [17]. Thus, evaluating the flow pattern of the IJV by Doppler ultrasonography could provide more information on the patient’s hemodynamics, blood loss, and response to venous resuscitation. The flow pattern of the IJV was recently proposed as a way to examine volume loss. A previous study examined IJV blood flow in blood donors after blood donation by Doppler ultrasonography and showed a decrease in the jugular pulsatility index (JPI) after blood donation. The JPI was calculated using the following equation: (Vmax-Vmin)/Vmax [18].
To the best of our knowledge, IJV Doppler ultrasonography has not been examined yet in trauma patients. Given the high mortality risk of bleeding in trauma patients and the significance of the rapid diagnosis of bleeding in these patients, the present study was conducted to examine the relationship between IJV Doppler findings and hypovolemic shock in trauma patients.
Materials and Methods
Compliance with Ethical Standards
The study was conducted after obtaining permission from the Research Council and approval of from the Ethics Committee of the Baqiyatallah University of Medical Sciences (IR.BMSU. REC.1398.300). Informed written consent was received from all the patients or legal guardians. Moreover, in all stages of the study, the provisions of the ethics statement in the Helsinki study and the principles of patient information confidentiality were observed.
Patients
This prospective observational was conducted between January 1, 2020, and December 30, 2020, on polytrauma patients admitted to Baqiyatallah al-Azam Hospital, Tehran, Iran.
The sample size was determined based on previous studies [18]. Using logistic regression analysis and values of α=0.05 and β=0.2, a sample of at least 30 people in each group was calculated. Purposive sampling was conducted. The sample comprised polytrauma patients (injury severity score [ISS]>15) aged 18-60 years old. All participants had been transferred to the hospital within one and a half hours after suffering the trauma, and none showed any symptoms of hemorrhagic shock at the time of admission. Hemorrhagic shock was defined as any of the following: SBP less than 90 mmHg, decreased urinary output to 30 mL/h, blood loss more than 750 mL, heart rate above 100/min or transfusion of >2 units of packed red blood cells (PRBCs) [19]. Moreover, patients with any of the following conditions were excluded from the study: pregnant patients; those with a direct penetrating or blunt injury to the right side of the neck (spine injury), known cardiac disease, pericardial effusion, pneumothorax, emergency thoracotomy, mechanical ventilation, flail chest, positive extended focused assessment with sonography for trauma (EFAST) results, hemoglobin (Hb) below 10 mg/dL, penetrating abdominal injury; and those who were taking vasoactive medicines.
Patient Evaluation
Upon admission, all patients were examined by an emergency physician and treated according to the Advanced Trauma Life Support guidelines. All vital signs were recorded, blood samples were taken for routine analysis, blood grouping and cross-matching were performed, and patients’ demographic information was recorded. The laboratory parameters studied were blood lactate level, bicarbonate level (HCO3), base excess (BE), blood pH, and Hb. Additionally, patients’ age, sex, injury mechanism, injury severity (based on ISS), the time elapsed between trauma and admission, and hospitalization duration before undergoing ultrasonography were examined and recorded. Patients’ loss of consciousness was evaluated using the Glasgow Coma Scale (GCS). An experienced radiologist (with more than 10 years of experience) performed IJV ultrasonography in all patients. Ultimately, the patients were divided into two groups: those who experienced hemorrhagic shock during the first 6 hours and those who did not. Finally, the data obtained from both groups were compared.
Ultrasound Evaluations
EFAST was conducted on all patients no more than 10 minutes after admission to the emergency room. In the absence of free fluid in the abdomen and pelvis, right IJV Doppler ultrasonography was conducted as well. Patients who were EFAST-positive were excluded from the study.
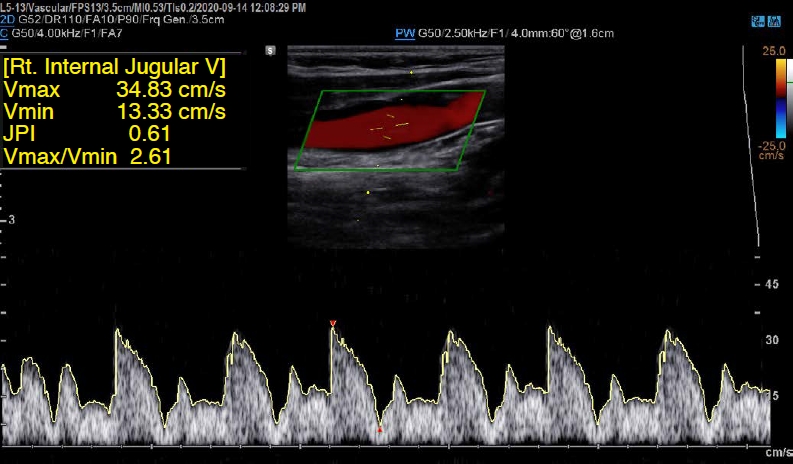
For Doppler ultrasonography, patients were placed in the supine position, and the IJV was identified in the axial plane using a linear probe. Measurements were taken using a 5 to 12-MHz linear probe of a Samsung HM70A ultrasound device (Samsung healthcare, Seoul, Korea). The probe was placed along the longitudinal plane, and the sample volume was determined to be one-third of the vein diameter, with an angle of insonation of 60° or less. After three similar cycles were recorded, the maximum and minimum flow velocities (Vmax and Vmin) of the IJV were determined (Fig. 1). Then, Vmax-Vmin and the Vmax/Vmin ratio were calculated. Finally, the JPI was calculated as (Vmax-Vmin)/Vmax.
Statistical Analysis
Statistical analyses were performed using SPSS for Windows version 22 (IBM Corp., Armonk, NY, USA) and MedCalc for Windows version 13 (MedCalc Software Ltd., Ostend, Belgium). The data were described in terms of mean, standard deviation, frequency, and percentage. The normality of the data was examined using the Kolmogorov-Smirnov test. The Student t-test, chi-square test, and Pearson correlation coefficients were used to measure the differences and compare the variables. Various parameters of the receiver operating characteristic curve were evaluated, and the areas under the curve (AUCs) were compared to evaluate the diagnostic performance. The significance level of the tests was considered 0.05. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (+LR), and negative likelihood ratio (-LR) of each of the parameters for the diagnosis of hemorrhagic shock were reported.
Results
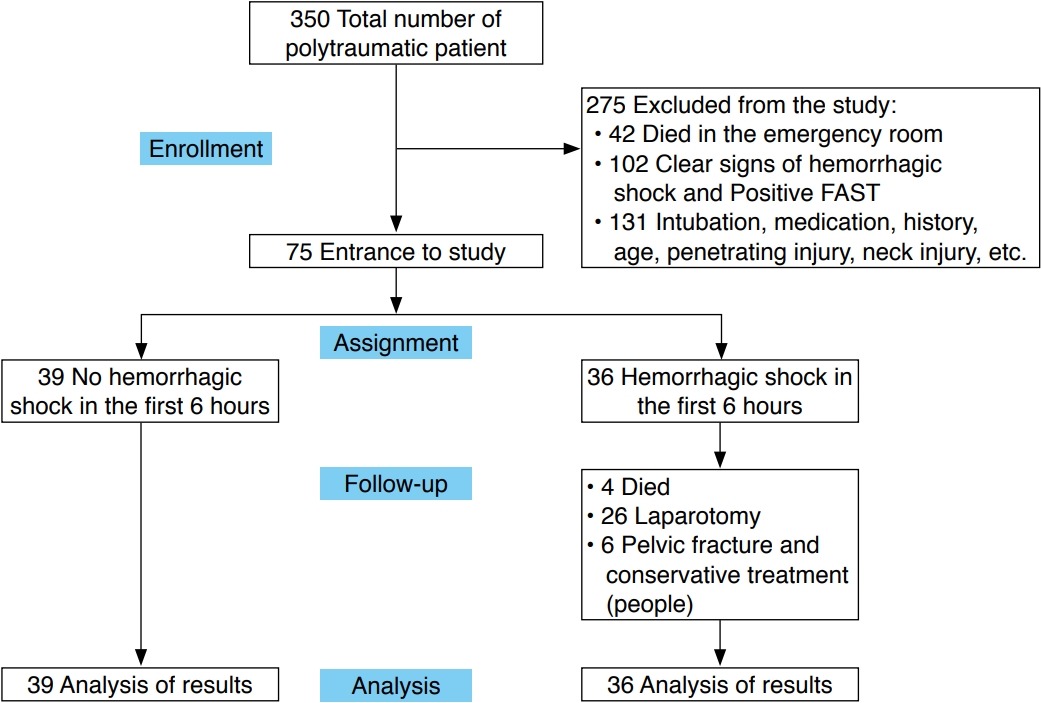
Out of 350 hospitalized polytrauma patients, 275 were excluded and 75 patients aged 19 to 57 years participated in this study. The flowchart of the study is presented in Fig. 2.
The basic characteristics of the patients from both groups are presented in Table 1. There were no significant differences between patients with and without hemorrhagic shock in terms of age, sex, mechanism of trauma, the time between trauma and hospitalization, and the time between admission to the emergency ward and undergoing ultrasonography (P>0.05).
Table 2 shows the results of vital signs, clinical parameters, and ultrasonography. The two groups did not differ significantly in terms of SBP, respiratory rate (RR), pH, GCS, PR, or Hb (P>0.05). Significant differences between the two groups were detected for other clinical parameters (SI and ISS), laboratory parameters (lactate level, HCO3, and BE), and ultrasound parameters (Vmin, Vmax-Vmin, and JPI).
The relationships of the JPI with various parameters in the patients in the two groups are presented in Table 3. Significant relationships were observed between the JPI and transfused PRBCs, BE, HCO3, actate, ISS, SI, and GCS in patients with hemorrhagic shock. There were no significant relationships for other variables. Significant relationships were found between the JPI and transfused PRBCs, BE, HCO3, lactate, ISS, and SI in the patients without hemorrhagic shock.
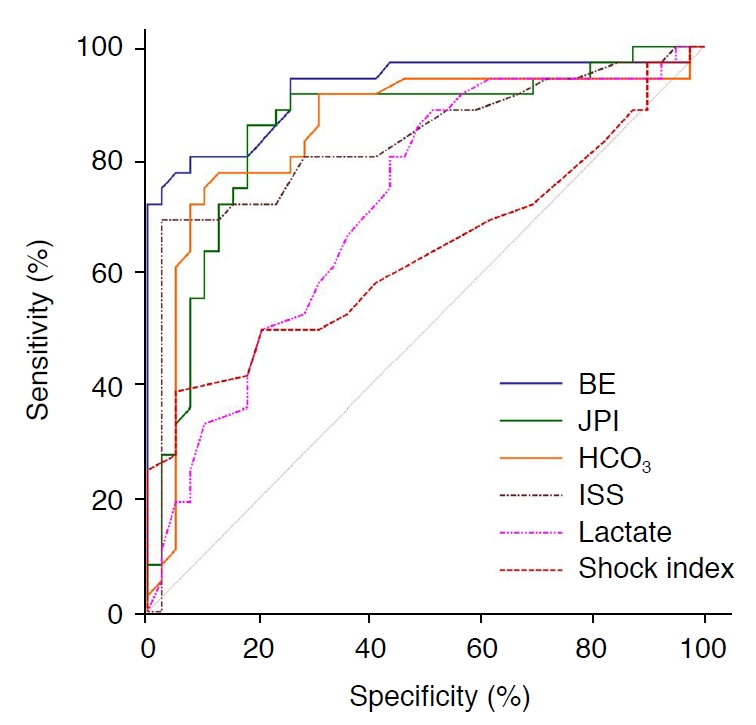
Table 4 presents the sensitivity, specificity, +LR, -LR, PPV, NPV, and AUC for each parameter that had significant differences between the two groups and was examined for the diagnosis of hemorrhagic shock. The best discriminant ability was shown by BE (AUC, 0.925), JPI (AUC, 0.853), HCO3 (AUC, 0.851), and ISS (AUC, 0.832) (P<0.001). Fig. 3 shows the comparison of the discriminant ability of various parameters based on the AUC.
Discussion
Conventional methods for quickly diagnosing bleeding in trauma patients are not reliable [5]. Rouhezamin et al. [18] showed that clinical indicators such as PR, SBP, and SI could not predict the early stages of hypovolemic shock in blood donors. Other studies have reported that clinical data and vital signs are unreliable indices for detecting the early stages of hemorrhagic shock [20,21]. The present study findings confirm those findings; specifically, there were no significant differences in SBP, RR, pH, PR, and Hb between patients with and without hemorrhagic shock, suggesting that these parameters do not reliably predict bleeding. Among laboratory tests, an increased base deficit indicates lactic acidosis and anaerobic metabolism due to impaired tissue perfusion. Previous studies have indicated that venous blood gases and lactate levels accurately predict volume loss and hypovolemic shock, but some of these indices are not accurate enough to detect small volumes of blood loss and are unavailable at the patient’s bedside [18,22-24]. In the present study, an increased base deficit was the best indicator of hemorrhagic shock; however, although this index is an acceptable prognostic factor in trauma patients, other factors (e.g., hypocapnia, hyponatremia, and acidosis) can affect it [25].
Ultrasonography is an alternative tool for the diagnosis of volume loss. Celik et al. [14] found no significant associations between the IVC diameter or aorta diameter in trauma patients and clinical signs or laboratory tests. Furthermore, Juhl-Olsen et al. [9] assessed blood donors and detected no significant relationships between the IVC diameter (measured using ultrasonography) and cardiac output or the hemodynamic response in the early hemorrhagic stages.
Pucheu was the first researcher to explain that the typical Doppler flow pattern of the IJV is pulsatile [26]. Cardiac output and intravascular volume affect the venous dynamics and waveform [17]. Blood loss also affects these factors. Reduced cardiac output and venous return were reported in cases of bleeding and volume loss even without clinical signs of shock. However, other compensatory mechanisms maintain the oxygenation of vital organs such as the brain [27]. As a result, blood flow to the brain increases, while absolute cerebral blood flow and cerebral venous flow are slightly reduced [28]. At the same time, absolute and relative extracranial peripheral blood flow (facial muscles) also decreases [29]. In other words, absolute IJV blood flow decreases after volume loss [18], thus reducing the difference between the maximum and minimum flow (Vmax-Vmin) as the pulsatility of the IJV (JPI) decreases.
In a comparison of blood donors and control participants, Rouhezamin et al. [18] showed that the JPI declined significantly after blood donation and provided an accurate prediction of bleeding (AUC, 0.711). Moreover, they showed that using this index simultaneously with clinical and laboratory parameters (SI and base deficit) could improve the discriminant ability (AUC, 0.868).
In the present study, patients with hemorrhagic shock and without hemorrhagic shock exhibited significantly different flow pattern parameters in IJV ultrasonography (including Vmin, Vmax-Vmin, and the JPI). The JPI of the patients with hemorrhagic shock was significantly lower than that of the patients without hemorrhagic shock. The JPI also had good discriminant ability, with high sensitivity and specificity for predicting the occurrence of hemorrhagic shock (AUC, 0.853).
The significant relationships between JPI and HCO3, BE, and lactate are reasonable, as previous studies have indicated the high diagnostic performance of these parameters. The JPI also showed a significant relationship with PRBCs transfused in the first 6 hours.
Overall, the results show that ultrasound parameters (JPI in the present study and IVC diameter in other studies [9,14]) are not associated with hemodynamic parameters. This is reasonable, as clinical and laboratory parameters do not accurately predict the early stage of hemorrhagic shock, and these parameters have shown variable sensitivity in previous studies [5,6].
Ultimately, the findings of the present study indicate that the IJV Doppler flow pattern evaluation has acceptable sensitivity and specificity for diagnosing hemorrhagic shock in trauma patients. Ultrasound devices are now available in all emergency departments and are easy to use. Therefore, IJV Doppler ultrasonography can be used with other clinical signs and blood gas parameter assessments as a supplement to the focused assessment with sonography for trauma examination.
The present study is the first to evaluate the function of IJV Doppler ultrasonography in diagnosing hypovolemic shock in polytrauma patients. Previous studies have focused on using IJV ultrasonography to assess hypovolemic shock after blood donation, with a focus on the diameter of the IJV [7,12,15,18]. Although blood donation can be used as a hemorrhagic shock model because the intravascular volume decreases rapidly after blood donation, vital signs change little during this process [30].
The present study has some limitations. For example, the relatively small sample that comprised only young and middle-aged patients could have influenced the results. However, the statistical analysis was not affected by this limitation. More accurate results might be obtained by carrying out more studies with larger samples.
IJV Doppler evaluations accurately predicted hemorrhagic shock in patients with polytrauma. IJV Doppler ultrasonography is a non-invasive, accessible, highly sensitive, and specific method for diagnosing early hemorrhagic shock. It can be routinely used in clinical examinations to identify patients at risk for hypovolemic shock.
 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



