

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
According to the ultrasound (US) lexicon of the Breast Imaging Reporting and Data System, hyperechoic lesions are defined as those with increased echogenicity in comparison with subcutaneous fat tissue [1]. Generally, well-circumscribed nodules that are intensely and uniformly hyperechoic are entirely composed of normal interlobular stromal fibrous tissue and are definitely benign [2]. However, hyperechoic lesions with iso- or hypoechoic areas larger than normal ducts or lobules should be approached with caution because the isoechoic or hypoechoic area may contain an occult carcinoma [2]. Moreover, it is difficult to identify hyperechoic lesions when they are surrounded by echogenic fibroglandular tissue. Although typical hyperechoic lesions with a distinct fat component on imaging are well known, some hyperechoic lesions are diagnosed as unexpected pathology, making the radiology-pathology correlation difficult.
This article reviews various breast lesions with unexpected hyperechogenicity along with other imaging findings, with a focus on the pathologic characteristics of hyperechogenicity and the goal of providing comprehensive knowledge for the differential diagnosis.
Benign Hyperechoic Lesions
Generally, a pure hyperechoic lesion has a 100% negative predictive value for malignancy [2]. Various pathologic conditions can cause benign lesions to be hyperechogenic. The presence of aggregated fibrous streaks, densely packed adipose tissue or clustered fibrous streaks, an intermixture of fibrous and adipose tissue surrounding adenomatous portions, or the presence of multiple small vascular channels can explain these pathologic findings [3]. Another possible explanation is heterogeneous stromal composition-that is, a high proportion of acellular stroma with stromal changes [4]. The lesions described below in this section are benign, but the diagnosis is difficult to predict, so the imaging-pathology correlation guides the lesion management.
Fibroadenoma
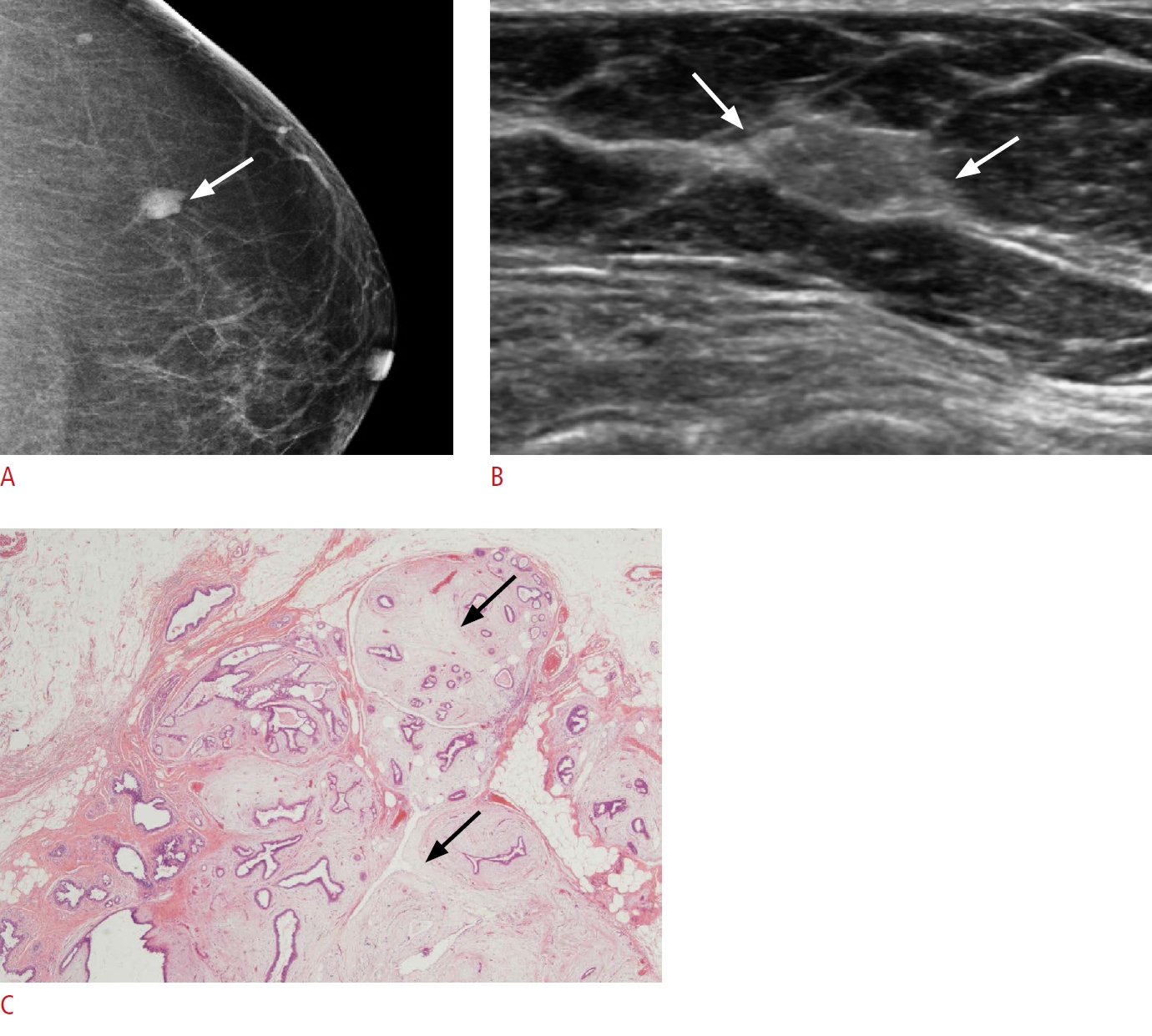
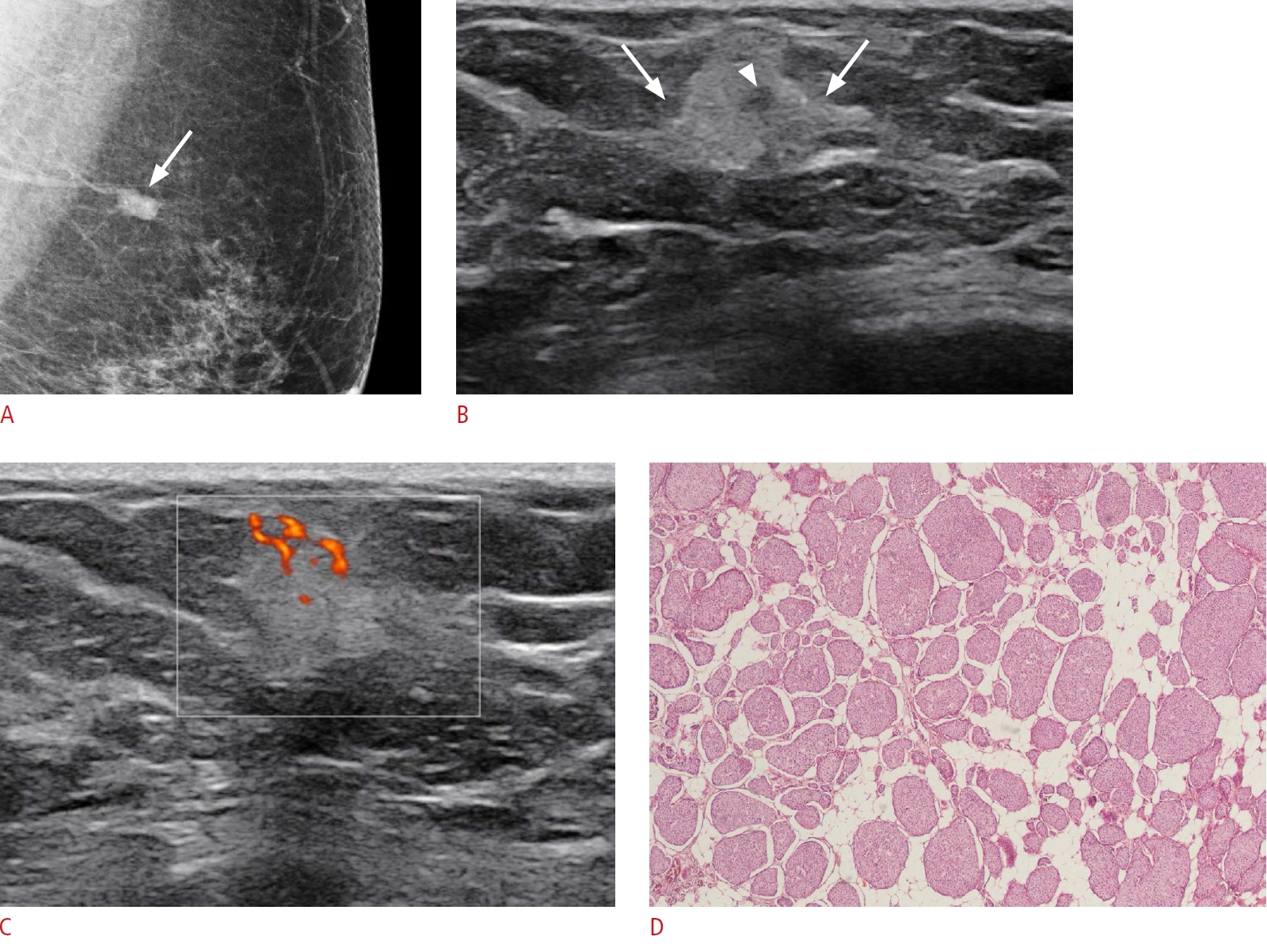
A smooth round or oval mass with homogeneous internal echoes is the typical US appearance of a fibroadenoma. There is a peripheral pseudocapsule adjacent to packed breast parenchymal tissue, allowing the surgeon to easily resect the mass. The echogenicity of fibroadenoma tends to be determined by its histologic composition. Microscopically, fibroadenoma arises from a terminal ductolobular unit (TDLU) and a variable amount of stroma and epithelial elements. Generally, a higher degree of epithelial elements is associated with a hypoechoic appearance, whereas a higher stromal composition yields a more echogenic appearance [4]. Moreover, the acellular stroma is more isoechoic and can even be mildly hyperechoic if the stroma is affected by sclerosis, hyalinization, myxoid change, or calcification [4]. In summary, a more hyperechoic appearance tends to be found in lesions with a higher stromal composition relative to the epithelial composition and lesser cellular stroma combined with stromal changes (Fig. 1).
Phyllodes Tumor
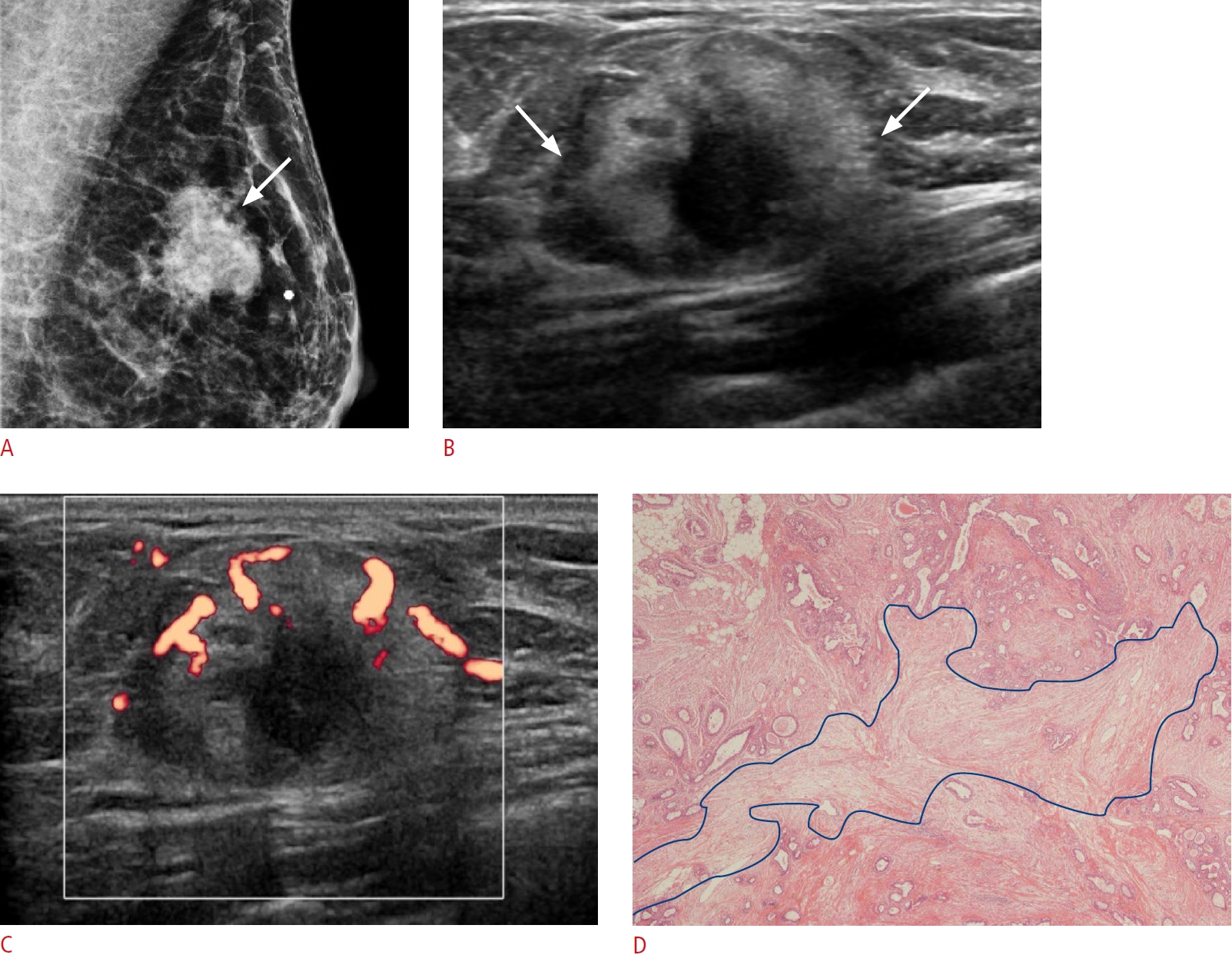
Phyllodes tumor is a rare fibroepithelial lesion of the breast with a proclivity for rapid growth. It is made up of epithelial and stromal components, with cleft-like cystic spaces acting as a diagnostic clue. This entity has a distinct leaf-like architecture with abundant cellular stroma, which distinguishes it from fibroadenoma and other stromal sarcomas [5]. Phyllodes tumors are classified as benign, borderline, or malignant based on their histopathologic features, such as the degree of stromal cellularity and atypia, mitotic count, and stromal overgrowth.
A benign phyllodes tumor resembles cellular fibroadenoma, while a malignant phyllodes tumor can be mistaken for primary breast sarcoma or spindle cell carcinoma. Distinguishing benign phyllodes tumor from fibroadenoma is difficult on core needle biopsy (CNB). Therefore, fibroepithelial lesions diagnosed using CNB are currently treated with either vacuum-assisted or open excision. Surgical excision is usually preferred because it enables negative margins in the event that the final diagnosis is a phyllodes tumor.
Adenosis
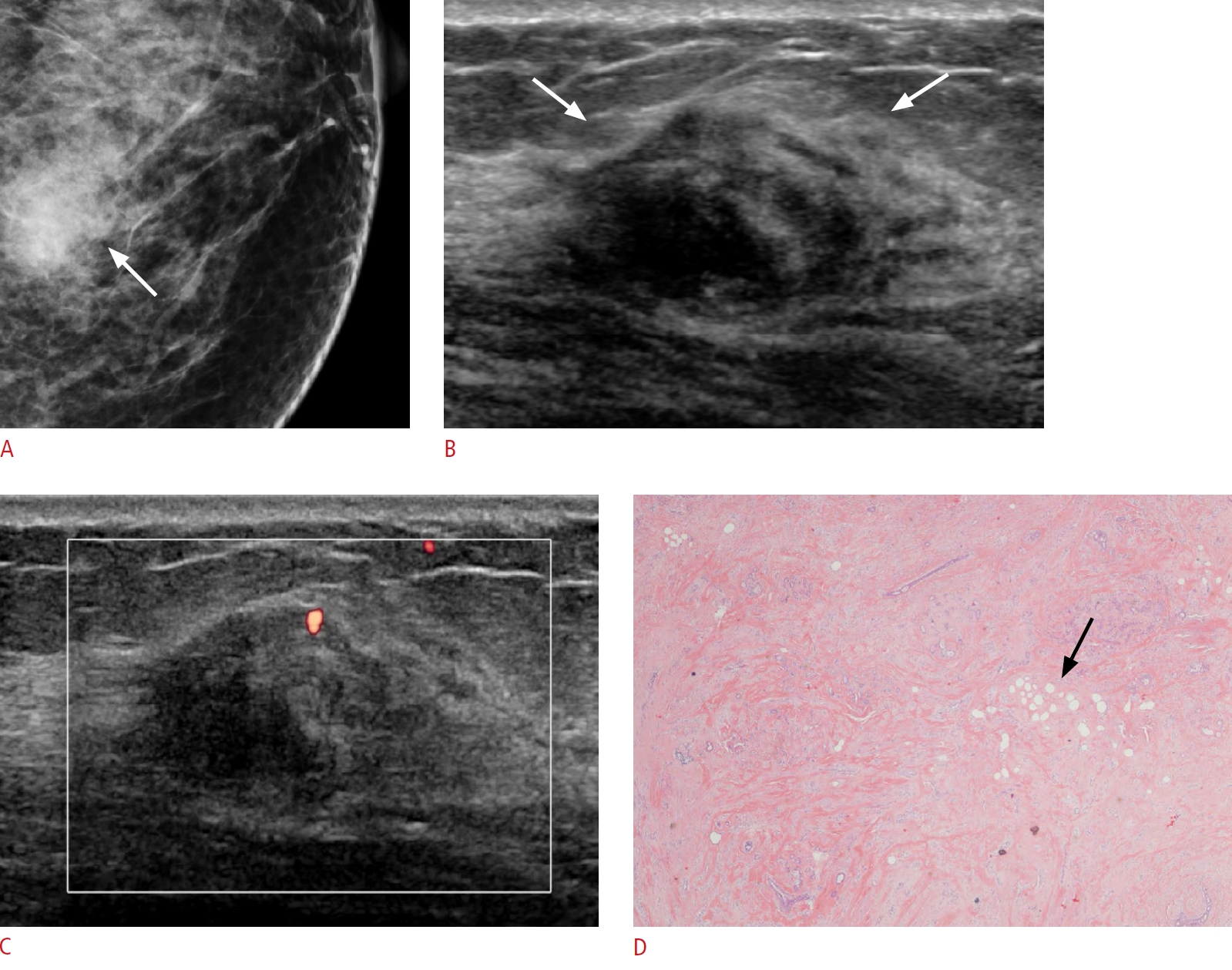
Adenosis of the breast is characterized by hyperplasia of all TDLU constituents (epithelial cells, myoepithelial cells, and connective tissue). Clinically, it may manifest as a slowly growing breast swelling. Pathologically, it is classified into three groups: sclerosing adenosis, blunt duct adenosis, and microglandular adenosis [7].
Adenosis has nonspecific US findings, with variable echogenicity, and hyperechogenicity of an adenosis tumor could be attributed to an increased extent of the interfaces between prominent glandular tissue and fibrosis (Fig. 3).
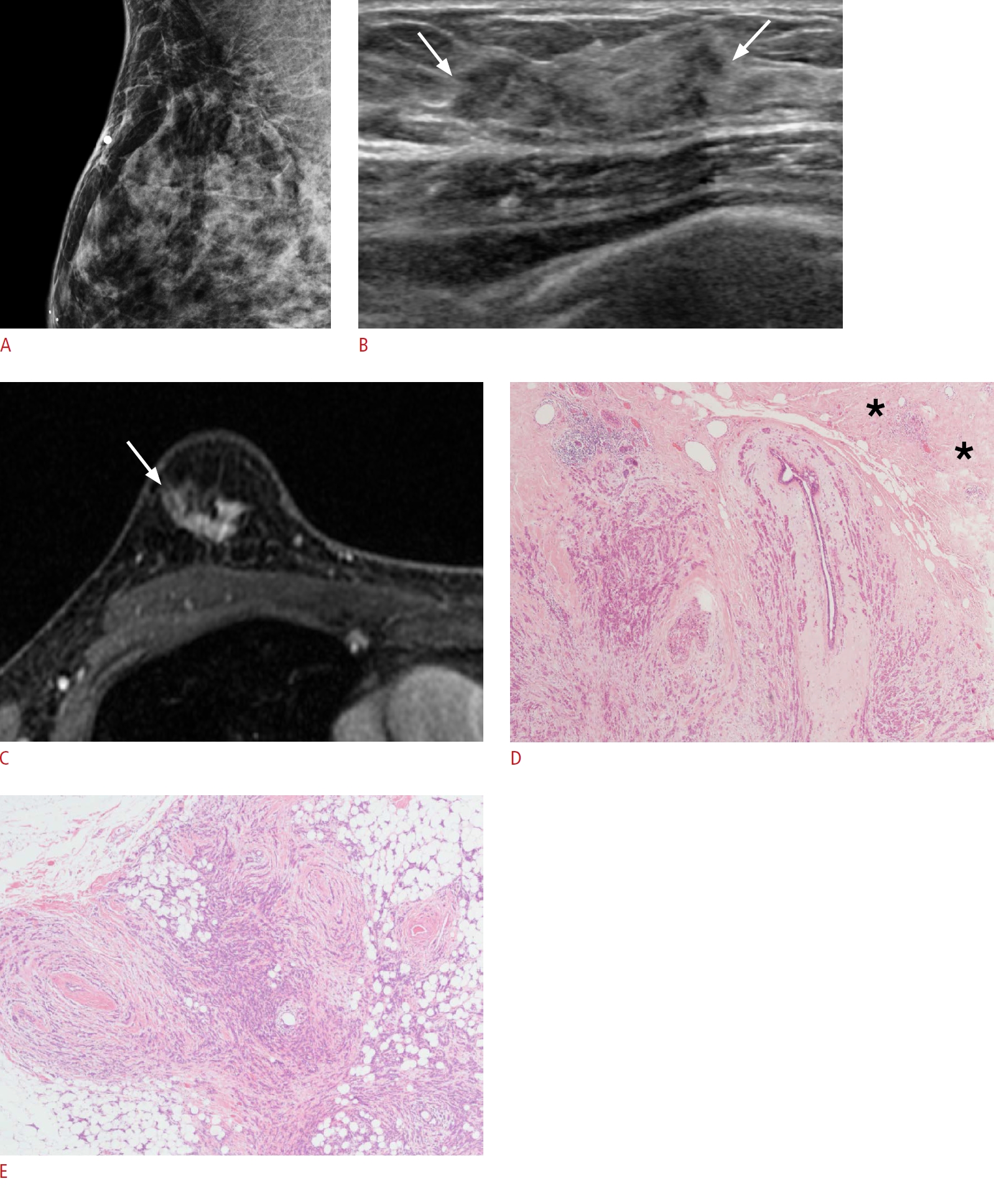
Myofibroblastoma
Myofibroblastoma is a rare benign spindle cell tumor that has myofibroblastic characteristics. These tumors have uniform spindle cells in short fascicular clusters and interspersed bands of hyalinized collagen. The spindle cells express vimentin, CD34, and desmin, but not S-100 protein nor cytokeratins [8].
The mammographic appearance of the tumor can be well-circumscribed or ill-defined, and it can be round, oval, or lobular in shape. The most common US features are a homogeneously hypoechoic well-circumscribed solid mass that may resemble a fibroadenoma [8]. The fat component and multiple internal tissue interfaces among fibrous tissue, fat, and cellular components in the tumor may be the cause of hyperechogenicity (Fig. 4) [9].
Malignant Hyperechoic Lesions
Malignant hyperechoic lesions are uncommon, but other suspicious US features, such as a non-parallel orientation and non-circumscribed margins, are usually present, indicating malignancy.
Malignant hyperechoic masses can be seen in two major types of US patterns. The first is a rim pattern, which consists of a hypoechoic area within the mass and a hyperechoic rim surrounding it. The central area is made up of tumor cells embedded in a dense stroma, and the hyperechoic surroundings are associated with tumor cells infiltrating into adipose tissue [10]. According to Linda et al. [11], a focal hypoechoic region surrounded by a hyperechoic area is more common in malignant lesions. Therefore, when a hyperechoic lesion is discovered in the breast, the presence of a hypoechoic area should be considered among the suspicious US findings. The other is a dispersed pattern with tumor cells infiltrating into the surrounding adipose or fibroglandular tissue with minimal desmoplastic reaction [10]. Sometimes this pattern makes the lesion difficult to find on US. Therefore, finding suspicious features of a corresponding area on mammography aids in the differentiation of malignant and benign hyperechoic lesions.
Invasive Ductal Carcinoma
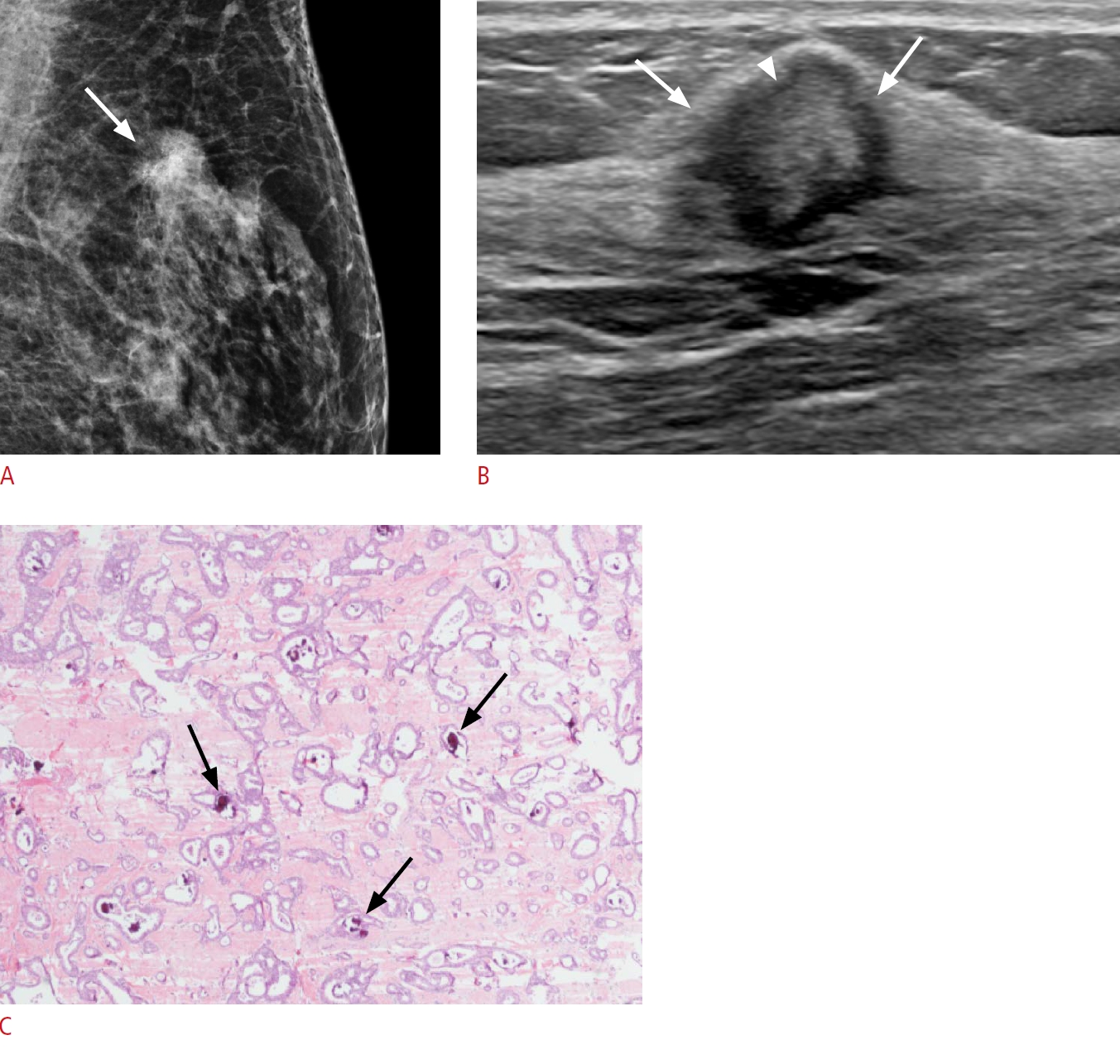
Because of the wide range of histological findings in invasive ductal carcinoma (IDC), mammographic and US findings are also diverse. The most common US finding is an irregular hypoechoic mass with a non-circumscribed margin. The internal echo of usual breast cancer is hypoechoic in the majority of cases, but hyperechoic masses can occur in rare cases. Malignant masses can be composed of tumor cells mixed with other tissue components with varying echogenicity, such as adipose tissue (Fig. 5), fluids (secretions, intercellular fluid, or blood), hemosiderin, and/or microcalcifications (Fig. 6) [10]. The complex intermixture of various elements is thought to play a role in hyperechogenicity on US. Another possible explanation is tumor cellular heterogeneity, such as a cribriform pattern, tubular structure, solid nests, and scirrhous pattern.
Invasive Lobular Carcinoma
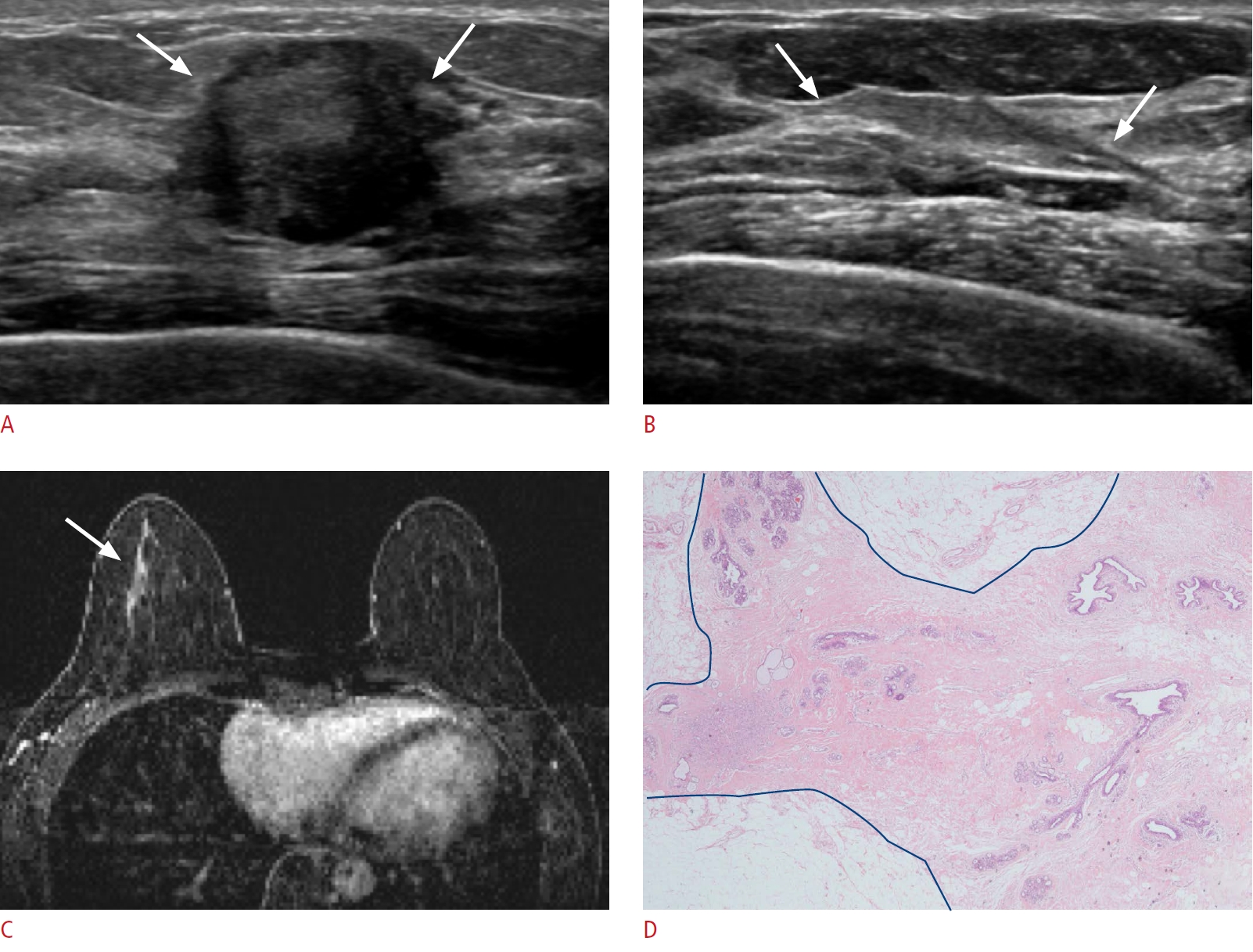
Invasive lobular carcinoma (ILC) is the second most common type of breast cancer, accounting for approximately 7%-10% of all cases. Microscopically, ILC is made up of malignant cells that grow in the mammary stroma and adipose tissue in a single-file fashion around normal breast ducts. On mammography, the most common finding is asymmetric density. However, ILC presents with nonspecific findings more often than other breast carcinomas, and it frequently exhibits multifocal and multicentrality, as well as no abnormality at all. The US findings range from no detectable lesion to a mass similar to IDC. US detectability depends on whether the tumor forms a mass and the relative proportion of the lesion that is diffusely infiltrating [12]. The most common US finding is a heterogeneous mass with irregular or indistinct margins and posterior acoustic shadowing [12]. According to Watermann et al. [13], hyperechoic and isoechoic patterns are more common in ILCs than in tumors of other histologic differentiation. These specific US findings could be explained in two ways by the distinct histologic growth patterns of ILC. First, ILC involves the increasing infiltration of the surrounding parenchyma as rows of single cells and in concentric rings around normal ducts, resulting in an increase in reflective surfaces and increased echogenicity with posterior acoustic shadowing [12,13]. In addition, the alternating repetition of tumor cells and intercellular fibrotic stroma could contribute to hyperechogenicity, as in the case presented herein (Fig. 7). Another plausible explanation is that the tumor can infiltrate adjacent fat tissue, increasing the echogenicity of the mass.
Mucinous Carcinoma
Mucinous carcinoma is an extremely rare type of IDC, accounting for <2% of all breast cancers. In this type of cancer, the tumor is made up of abnormal cells that "float" in pools of mucin. Pathologically, mucinous carcinoma is classified into pure mucinous carcinoma and mixed mucinous carcinoma based on the mucinous component.
On mammography, mucin appears with increased density with a well-circumscribed or microlobulated mass, but the margin can be obscured at times. On US, it has a heterogeneous echo with a mixed internal solid and cystic area and posterior acoustic enhancement. Moreover, extracellular viscous mucin and microcalcifications may explain the hyperechogenicity (Fig. 8) [14]. When the suspicious mass has increased echogenicity with a relatively circumscribed margin on US and high signal intensity on T2-weighted magnetic resonance imaging, mucinous carcinoma should be considered (Fig. 8D).
T-Cell Lymphoma
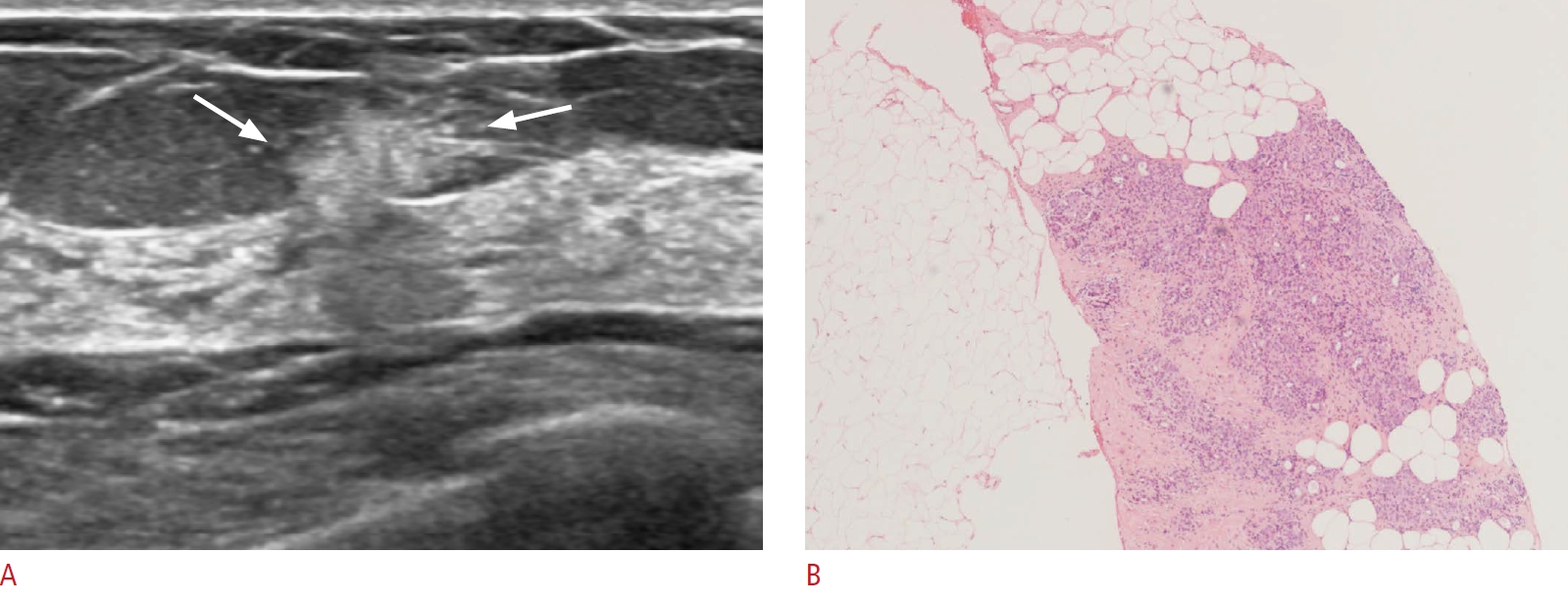
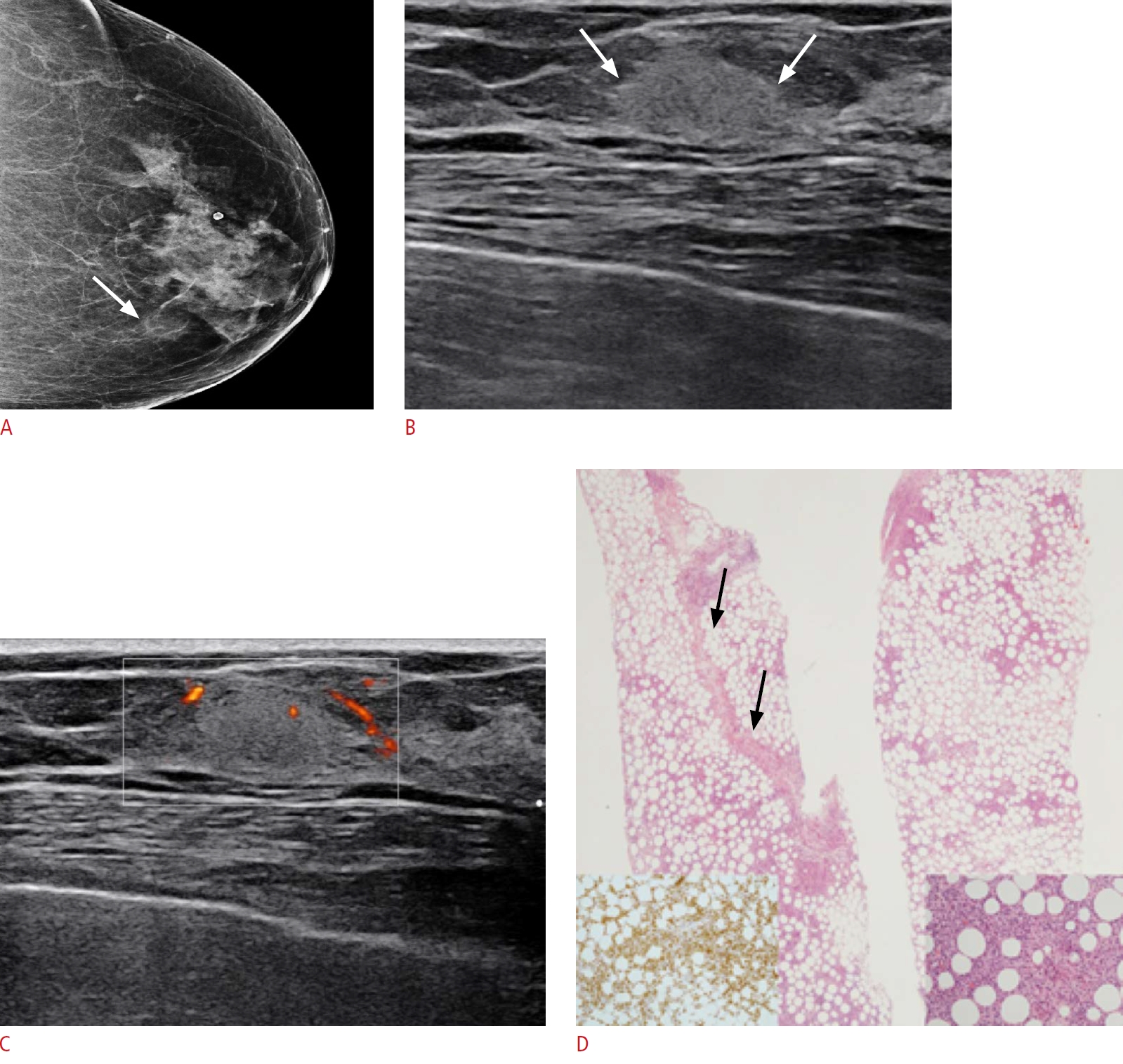
Primary breast lymphoma (PBL) is a rare hematologic malignancy, accounting for only 0.05%-0.53% of all breast malignancies [15]. PBL is mostly non-Hodgkin lymphoma (specifically, high-grade B-cell lymphoma). Most cases of PBL were shown to be oval-shaped and high-density masses on mammography. A hypoechoic, homogeneous or heterogeneous well-defined mass is the most common US finding in malignant lymphoma of the breast. According to Yang et al. [16], a hypervascular irregular mass with indistinct margins or an echogenic boundary is an even rarer subset of PBL and has a poorer prognosis than the B-cell type. T-cell lymphoma involving the breast is considered an aggressive disease. T-cell lymphoma shows diffuse infiltration of the normal architecture by medium-sized to large cells with pleomorphic nuclei (Fig. 9). Invasion of the breast of T-cell lymphoma usually presents as a bilateral involvement, mimicking mastitis. The hyperechogenicity of the tumor may be explained by tumor cells infiltrating the breast parenchyma and fat (Fig. 9).
Postchemotherapy Changes
In locally advanced breast cancer and inflammatory breast cancer, neoadjuvant chemotherapy (NAC) is the treatment of choice before surgical treatment. A pathologic complete response has been considered as the most important predictor of NAC outcomes and has emerged as a surrogate prognostic marker in many clinical trials. During NAC, the change in tumor echogenicity can predict a pathological response in monitoring. As a result of NAC, the tumor becomes composed of tumor cells with fibrosis, collagenization, and microcalcifications in the stroma. These multiple reflective surfaces can cause hyperechogenicity on breast US (Fig. 10) [17]. Therefore, an increase in echogenicity during NAC may indicate a more effective tumor response. Dobruch et al. suggested that persistent tumor hypoechogenicity after three courses of NAC predicts a poor response to treatment [18].
Metastasis
Metastasis to the breast from extramammary neoplasms is infrequent. A correct diagnosis of breast metastasis is critical because the treatment and outcomes of primary and secondary breast malignancies differ [19].
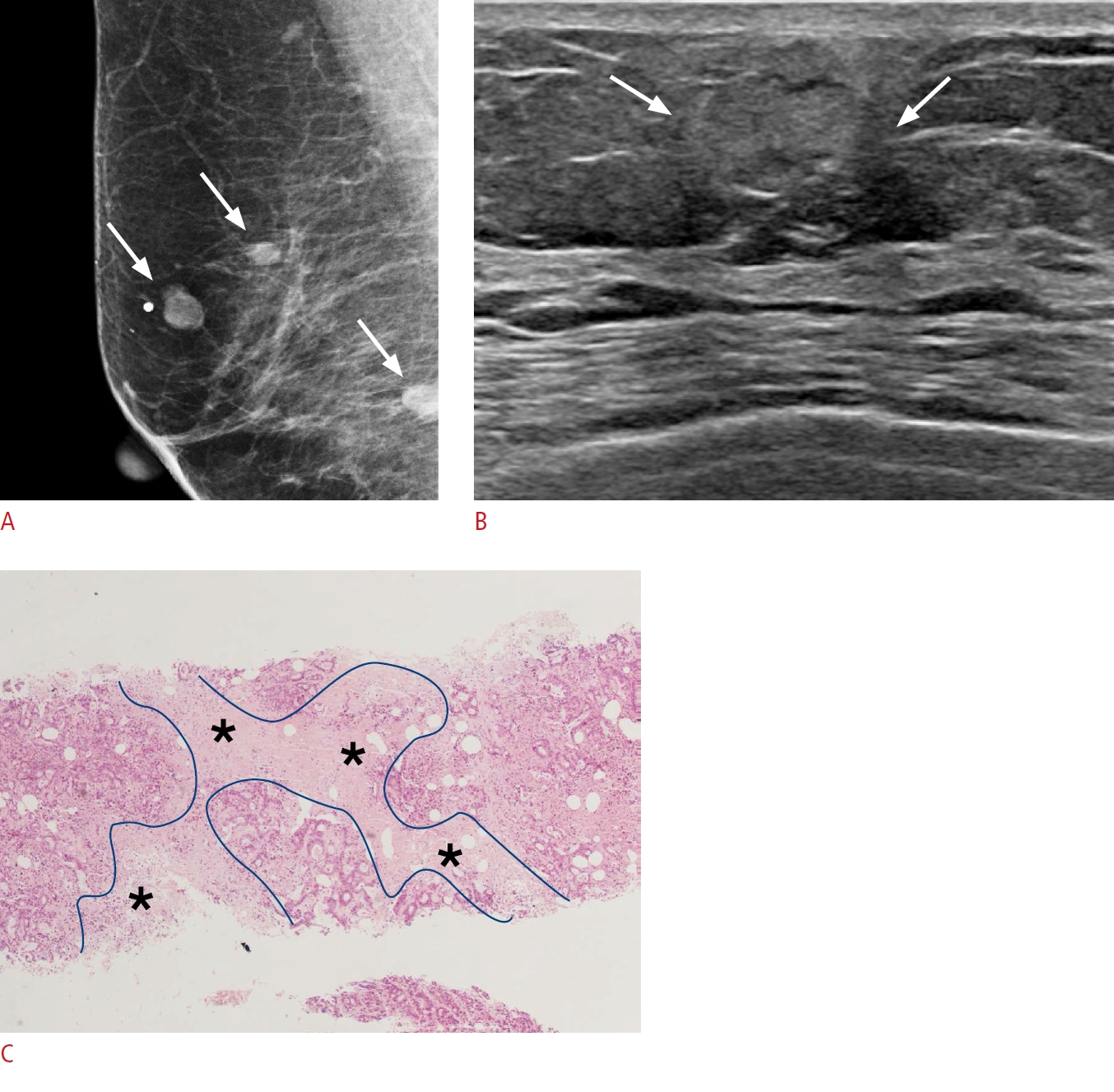
The most common mammographic appearances of metastatic breast cancer are one or more well-circumscribed masses without spiculation, calcifications, or other signs of a surrounding desmoplastic reaction that characterize primary breast cancer. The characteristic US findings are a hypoechoic, circumscribed mass with a round or oval shape. However, various US findings have been reported, including circumscribed or not circumscribed hyperechoic or hypoechoic solid masses with acoustic shadowing or enhancement [19]. In metastatic breast lesions, tumor cells infiltrating adipose tissue, hemorrhage with hemosiderin deposition (melanoma), papillary fronds of the tumor surrounded by extracellular fluid (papillary serous carcinoma), and necrosis can exhibit hyperechogenicity on US (Fig. 11) [20].
Conclusion
Hyperechogenicity on US does not guarantee benignity, and various breast lesions exhibit increased echogenicity. The pathology of hyperechogenicity indicates heterogeneity in tumor components, which increases the quantity of ultrasonic reflective surfaces. This means that hyperechoic tumors consist of an intermixture of various elements such as tumor cells or stroma with different cellularity, stromal changes, adipose tissue, microcalcifications, and fluid. However, to avoid missing malignant hyperechoic lesions, it is important to identify suspicious US or corresponding mammographic findings. A comprehensive knowledge of hyperechoic breast lesions helps in minimizing unnecessary examinations, making the correct diagnosis, and carrying out the appropriate management.

 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



