

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Nerve entrapment syndromes are frequently associated with structural abnormalities, such as compression and displacement [1]. They generally have a typical clinical presentation, which may begin with paresthesia and distal numbness and often progresses over time to muscle weakness and muscle wasting, depending on the extent of axonal damage at later stages [2]. In addition to patientsŌĆÖ clinical presentation, imaging modalities are increasingly being used to accurately assess nerve entrapments.
Magnetic resonance imaging (MRI) is useful for dedicated nerve entrapment assessment in a focal region, especially where ultrasonography (US) has limited access, but in most cases, US is an appropriate method to provide an overview of the entire length of the nerve. The progressive refinement of broadband transducers with high frequencies and improved near-field resolution has enhanced the potential of US to evaluate a variety of nerve entrapment syndromes [3]. US can define the level of nerve entrapment, at which MRI can then generate an overview to exclude possible secondary causes of entrapment, such as articular ganglia. Electromyography allows the assessment of nerve function, but does not precisely determine the type and degree of change.
Measuring the nerve's cross-sectional area (CSA) is one of the most important tools in the diagnosis of nerve entrapment syndromes. However, a defined CSA value for each peripheral nerve is still missing and a frequent point of discussion because it may differ in patients according to age, sex, physical habitus, comorbidities such as type 2 diabetes mellitus, or the imaging modality used (e.g., MRI or US) [4-7]. Furthermore, frequent work with oneŌĆÖs hands or fingers, such as among professional musicians, seems to lead to greater CSAs (e.g., in the median nerve) [8].
This article will focus on the diagnosis of the most common nerve entrapment syndromes via US, with particular attention paid to imaging landmarks and morphological features.
Pathophysiology and Sonographic Morphology of Nerve Compression
The main mechanism of nerve injury in compression is degradation and thinning of the myelin sheath due to compressive forces resulting in microvascular damage, while the morphology and neuromuscular junctions remain intact [9,10]. Mild degrees of compression may obstruct venous flow, causing congestion and edema, while more severe and consistent compression results in arterial ischemia. Prolonged or repetitive compression results in inflammation, fibrosis, and demyelination. Loss of myelination leads to disruptions in the speed of axonal signaling, and at its most severe can result in a partial or complete block of action potentials through the affected nerve segment. With persistent compression, the combination of these factors may lead to axonal degeneration. This portends a poorer prognosis and more prolonged recovery; remyelination may take a matter of weeks, while axonal regrowth is glacially slow, at approximately 1 mm/day [11,12].
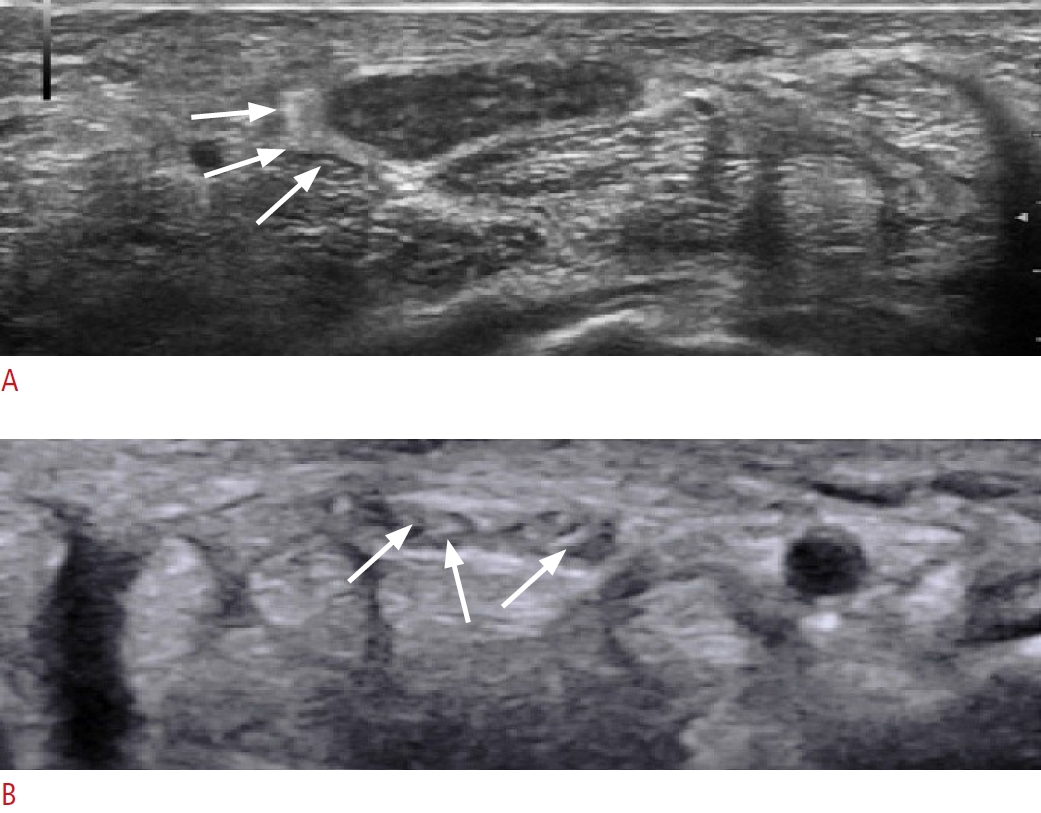
These changes in the nerve lead to typical appearances on US. A normal nerve has a typical honeycomb-like appearance with hypoechoic nerve fascicles and hyperechoic interfascicular perineurium [13]. With entrapment, this appearance on US changes to an irregular and blurred appearance with echogenic perineural fibrosis and the loss of fascicular echotexture [14]. Initially, the nerve often appears hypoechoic and swollen, which can change over time in chronic entrapment to intraneural fibrotic changes with echogenic spots and, therefore, a more echogenic appearance of the nerve, finally leading to the presentation of a smaller CSA due to edema regression (Fig. 1).
Nerve swelling can be measured by the CSA, which is increased in cases of focal compression and entrapment. Therefore, a measurement proximal to the entrapment level and a measurement at the maximal CSA at the compression site is recommended. This procedure enables the calculation of delta (i.e., difference) values, which allows an objective gradation of nerve thickening in nerve entrapment by US [15,16].
Median Nerve
Carpal tunnel syndrome (CTS) is the most common entrapment neuropathy, affecting 9% of women and 0.6% of men, and it is responsible for significant morbidity and occupational absence [17]. It is caused by compression of the median nerve at the wrist as it passes through a space-limited osteofibrous canal. The syndrome is characterized first by intermittent, nocturnal paresthesia and dysesthesia that increase in frequency and occur during waking hours. Subsequently, loss of sensation develops along with weakness and thenar muscle atrophy later in the disease course, which result from extensive axonal degeneration. This sequence of symptoms is quite typical and rarely occurs in disorders other than CTS [18,19].
By allowing direct visualization of the compressed nerve, US provides additional information to that obtained from clinical tests and electrodiagnostic tests and can therefore depict possible causes of secondary CTS and describe anatomical variants, such as a bifid median nerve or a persistent median artery of the forearm, as well as space-occupying lesions, including tenosynovitis and ganglion cysts [20].
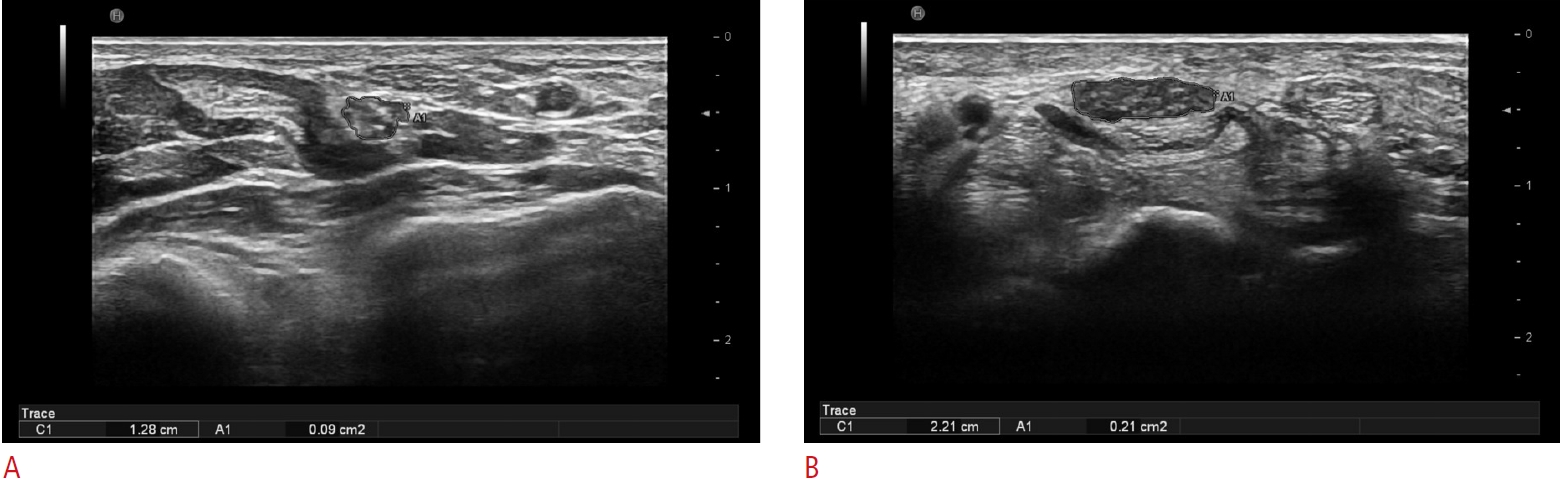
As in other nerve entrapment syndromes, US is a suitable method to determine CSA values. Because of the variability of CSA values of the median nerve, it has been proposed to present CSA ratios as a convenient method. A study by Klauser et al. [15] included 643 wrists of 427 patients with a CTS diagnosis based on clinical and nerve conduction studies. CSA measurement of the median nerve was performed at the carpal tunnel level and at the pronator quadratus muscle level. Two parameters were calculated: delta (Ōłå- CSA), which referred to the difference between proximal and distal measurements, and the ratio (R-CSA), calculated by dividing the distal measurement by the proximal measurement. They found cutoff values for Ōłå-CSA and R-CSA of 6 mm2 and 1.7, respectively, to distinguish mild from moderate disease, and 9 mm2 and 2.2, respectively, to distinguish moderate from severe disease (Fig. 2).
Besides the constriction of the main nerve, smaller nerve branches can also be affected by entrapment, such as the palmar cutaneous branch, which provides sensation at the thenar eminence. It emerges in a variable location from the proximal aspect towards the transverse carpal ligament and divides into a lateral and a medial portion. The lateral portion supplies the recurrent motor branch for the thenar muscles, whereas the median portion supplies two common volar digital nerves for the index and middle finger [21]. These nerve branches may also be affected in CTS and can be injured during carpal tunnel surgery or entrapped by scarring [22]. US can visualize these small nerve branches, enabling US-guided treatment as well.
If normal CSA values are detected on US, further examination of the median nerve towards the elbow is recommended, at which level entrapment due to hematomas, biceps tendinosis, and bicipitoradial bursitis might be the cause of entrapment.
Special Forms
The presence of anastomoses may increase the risk of iatrogenic injury during surgical procedures and make it difficult to interpret electrophysiological studies in the diagnosis of neuropathies. These anatomical variations must be differentiated from incomplete nerve lesions, since clinically, variations in the innervation of these small muscles are very important in the sense that, even with a complete lesion of the median or ulnar nerves, some of these muscles may or may not be paralyzed, which may lead to the erroneous conclusion that the nerve is not affected by a complete lesion [23].
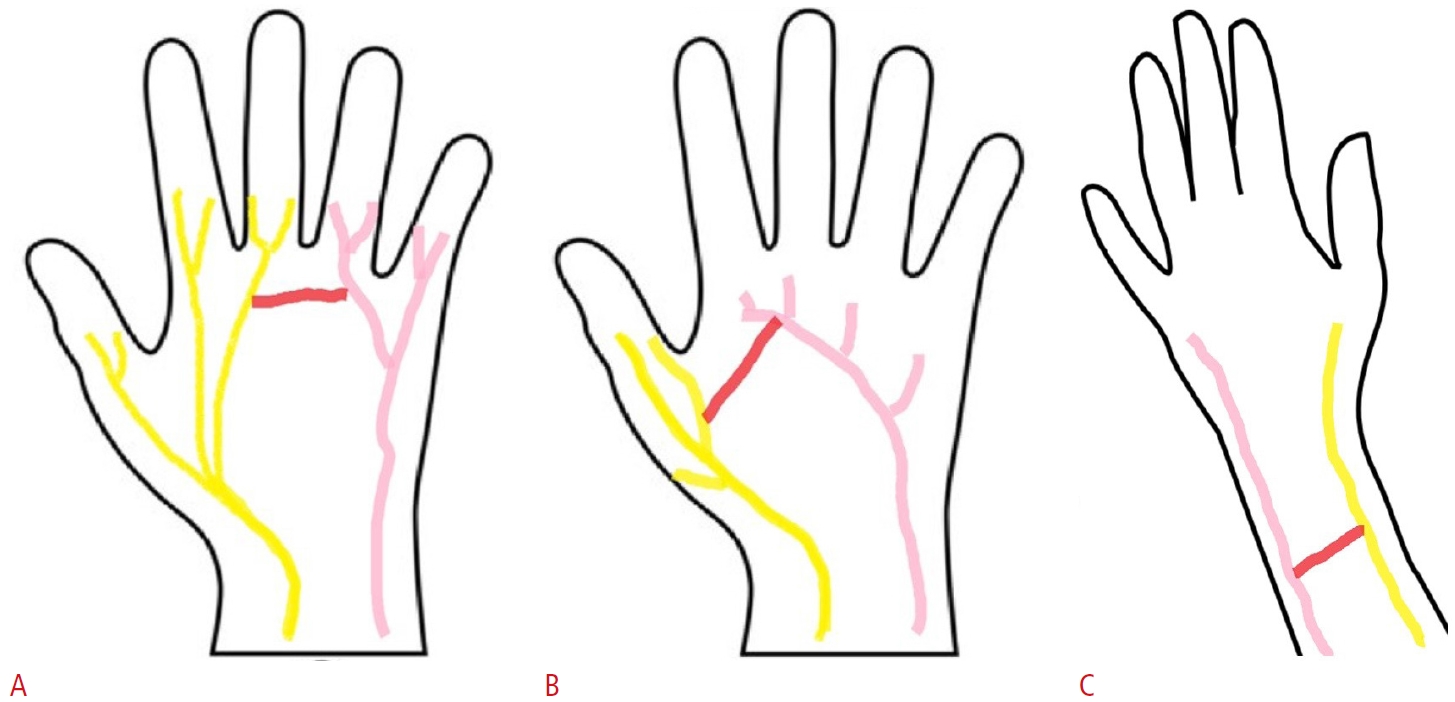
Unfortunately, there is not much literature available regarding the clinical implications of these anastomoses. Publications on this would be desirable. Nevertheless, a profound knowledge of these anastomoses is essential for the accurate interpretation of findings and for reducing the risk of iatrogenic injuries during surgical procedures (Fig. 3).
Martin-Gruber Anastomosis
In a study by Sur et al. [24] the Martin-Gruber anastomosis (MGA) occurred with a prevalence of 15.7%. The MGA emerges as a communicating branch in the cubital fossa from the main trunk of the median nerve, crosses superficial to the flexor digitorum superficialis or flexor digitorum profundus muscles, and then joins the ulnar nerve. The MGA has mainly been reported to supply motor innervation to the thenar, hypothenar, and dorsal interosseous muscles; however, some sensory fibers have also been identified with possibly variable clinical presentations [25,26].
Riche-Cannieu Anastomosis
The Riche-Cannieu anastomosis (RCA) occurs with a prevalence of 55.5% [25]. The RCA is a palmar anastomosis between the recurrent branch of the median nerve and the deep branch of the ulnar nerve, combining fibers of the ulnar nerve with those of the median nerve, leading to innervation of the thenar muscles [23].
Berrettini Anastomosis
The Berrettini anastomosis (BA) is an ulnar-to-median sensory nerve connection with a reported prevalence of 61% [25]. With its superficial position and close relation to the flexor retinaculum, usually at the region of the third digit, it is particularly vulnerable to iatrogenic injuries. While the BA is usually clinically silent, it may be associated with atypical patterns of sensory innervation, leading to a complex neurological assessment and unexpected patterns of sensory disturbance [27,28].
Ulnar Nerve
Ulnar neuropathy, often occurring at the elbow, is the second most common mononeuropathy seen in outpatient neurology settings [29]. Throughout its course, compression might occur in several locations; therefore, the nerve must be scanned over its entire course. Proximal compression might occur at the arcade of Struthers, a fibrous band running from the medial head of the triceps to the medial intermuscular septum, before the nerve passes through the epicondylar (ulnar) groove, located between the medial epicondyle and the olecranon. An anomalous anconeus epitrochlearis muscle overlying the ulnar nerve and extending between the olecranon and medial epicondyle may sometimes be a source of compression in this region. The cubital tunnel is located just distal to the elbow joint, and it is defined by the medial collateral ligament and the thickened fascia known as the Osborne (arcuate) ligament. This ligament lies between the medial and ulnar heads of the flexor carpi ulnaris and can also lead to entrapment of the nerve (Fig. 4).
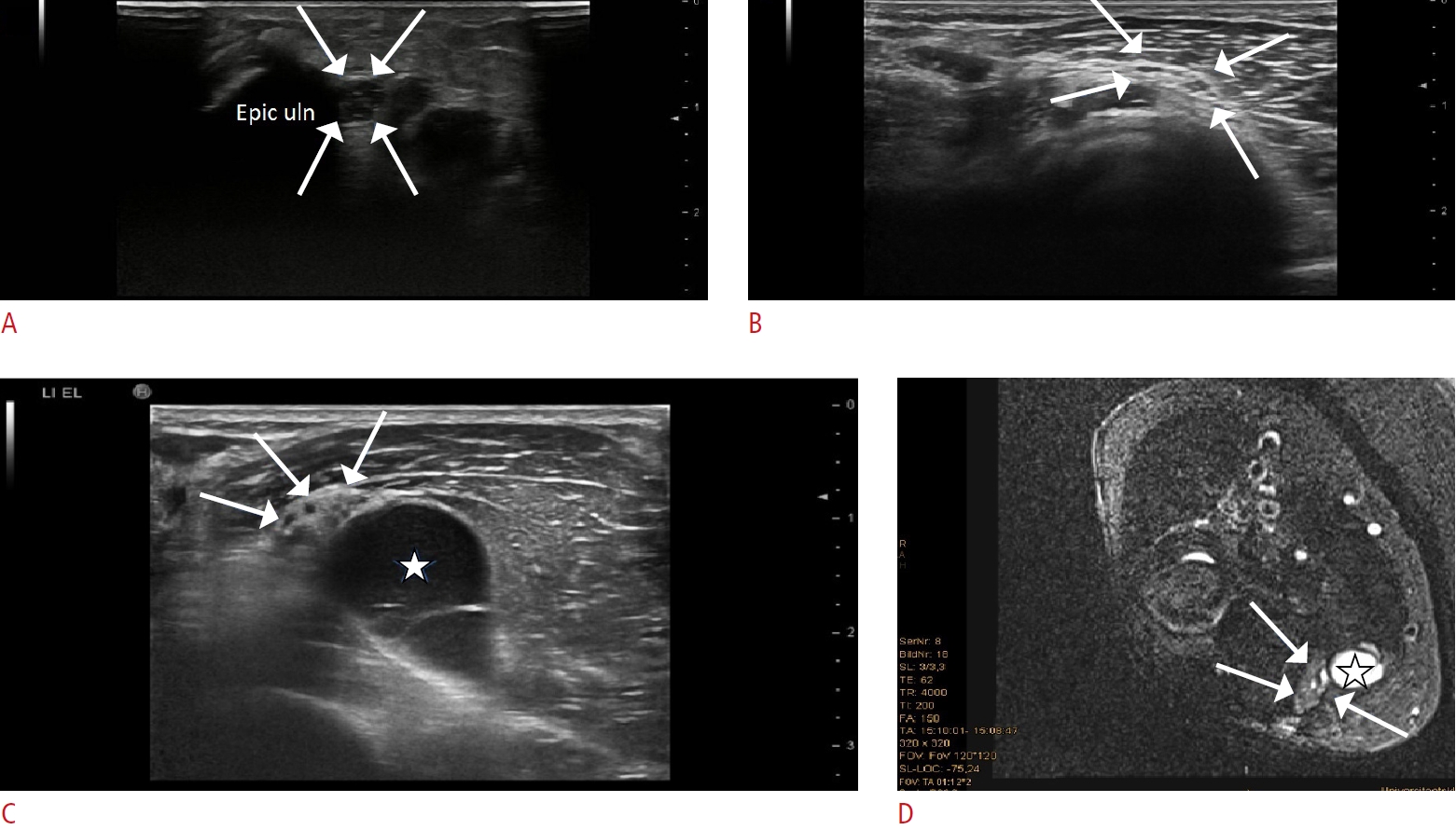
The normal ulnar nerve CSA at the elbow is 8 mm2 to 11 mm2, with larger values suggesting focal compression (Fig. 5A) [30]. However, the diagnosis of cubital tunnel syndrome is not only based on the CSA but also on textural analysis of the nerve, and a thickened and hyperechoic epineurium might be one of the earlier changes, before an increased cubital-to-humeral nerve area ratio occurs (Fig. 5B) [31,32].
Ganglia arising from the elbow joint can also lead to cubital tunnel syndrome (Fig. 5C, D). Distal compression might occur within the Guyon canal. In Guyon canal syndrome, the ulnar nerve is compressed, leading to paresthesia and later complaints of motor abnormalities in the distribution of the fourth and fifth digits, as well as weakness in the midpalmar muscles. Guyon canal syndrome most commonly results from compression of the nerve within the canal by a space-occupying lesion, such as a mass, varix, ulnar artery pseudoaneurysm, or ganglion cyst or extrinsic compression, such as by handlebars in avid bicyclists or in players of golf and racquet sports [33-36].
US has emerged as a reliable method for assessing ulnar neuropathy.
Radial Nerve
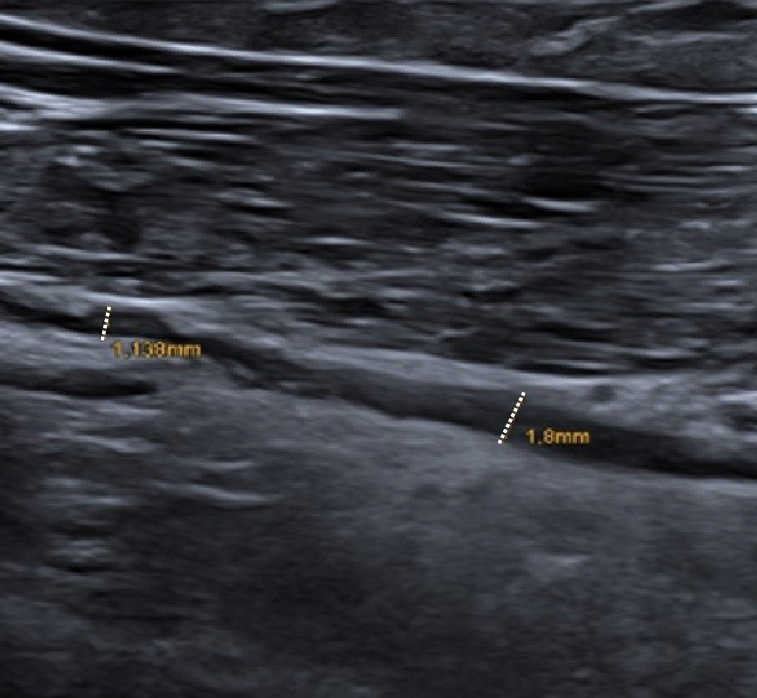
The annual incidence of this peripheral compressive neuropathy is approximately 0.03% as compared with CTS, which ranges between 0.1% and 0.35% [37,38]. Radial tunnel syndrome is an uncommon condition caused by entrapment of the radial or posterior interosseous nerve [39,40]. It presents primarily as pain within the mobile wad, approximately 3-5 cm distal to the lateral epicondyle, for which reason lateral epicondylitis is a major possibility considered in the differential diagnosis. Various compressive etiologies have been described, including fascial bands, radial recurrent vessels, the proximal edge of the supinator, and various space-occupying lesions (ganglions, hemangioma, lipoma, synovium, or accessory muscle). The most common site of compression is the arcade of Frohse (Fig. 6).
US can be used to assess the CSA of the nerve and therefore provide information about the grade of entrapment; however, often only a minor focal swelling or, on the contrary, a long-distance diffuse thickening might be observed.
Dong et al. [41] described the normal CSA values of the posterior interosseus nerve as follows: 1.6 mm2 at 1 cm proximal to the arcade of Frohse and 1.8 mm2 at 1 cm distal to the arcade of Frohse. However, no clear cutoff value has been established for pathologic nerves [42].
Entrapment of the superficial branch of the radial nerve may occur in the distal forearm, leading to a condition known as Wartenberg┬┤s syndrome. The causes of nerve entrapment include compression by a bracelet, watch, or handcuff and irritation from an adjacent metal implant after fracture. It may also be associated with de QuervainŌĆÖs tenosynovitis [43]. Symptoms include numbness, tingling, burning, and pain on the back or side of the hand at the base of the thumb. Since the nerve branch is sensory there is no motor impairment.
Sciatic Nerve/Piriformis Syndrome
Piriformis syndrome is an underdiagnosed entity characterized by pain and/or dysesthesia in the buttock area, hip, or posterior thigh and/or radicular pain due to non-discogenic sciatic nerve entrapment in the subgluteal space [44,45]. Entrapment may occur due to hypertrophy of the muscle or an anomalous course of the sciatic nerve [45,46]. Piriformis syndrome involves a constellation of symptoms that include low back or buttock pain referred to the leg, which is often underdiagnosed and mistaken for more common disorders, including facet arthropathy, sacroiliitis, lumbar disc disease, and radiculopathy [47]. US is a feasible method to measure the thickness of the piriformis muscle, as well as the CSA and course of the sciatic nerve of the pathological site in comparison to the healthy side (Fig. 7) [48].
Wu et al. [49] compared imaging parameters between piriformis syndrome patients and healthy volunteers; both the piriformis thickness and the sciatic nerve diameter on the abnormal side of patients were significantly greater than those of healthy volunteers (thickness: 21.5 vs. 18.3 mm and diameter: 7.6 vs. 5.9 mm).
Lateral Femoral Cutaneous Nerve
The lateral femoral cutaneous nerve (LFCN) is a sensory nerve that originates from the lumbar plexus at L2/L3, which is characterized by high anatomic variability, especially at the level of the inguinal ligament and the anterior superior iliac spine [50,51].
Meralgia paresthetica is a disorder related to the entrapment of the LFCN. Patients usually complain of burning pain and/or dysesthesia located at the anterolateral thigh, which may radiate to the knee. Due to the sensory nature of the nerve, there are no changes in any muscles. Obesity, diabetes mellitus, pregnancy, and advancing age are risk factors [51,52].
The course of the LFCN is very superficial; thus, it is susceptible to irritation resulting from causes such as too-tight clothing, especially in obese patients. Moreover, at the site where the LFCN pierces the fascia lata, it may become damaged by a tension mechanism (abrupt hyperextension of the hip) or a compression mechanism (a prolonged standing position). Iatrogenic damage may be caused by a direct anterior approach for total hip arthroplasty. The occurrence of nerve injuries in such procedures is very variable throughout the literature, ranging from 14.8% to 81%; therefore, this represents a frequent and underestimated presentation [48,53].
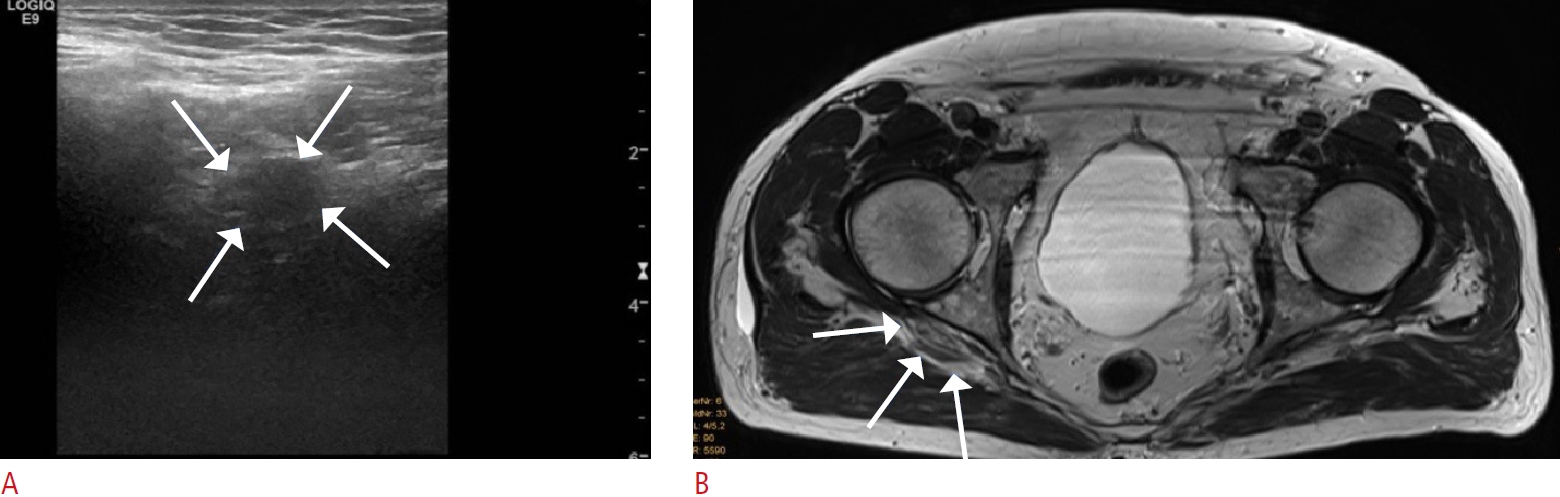
US findings in positive cases include nerve enlargement (mean, CSA 9 mm2 vs. 3 mm2 in normal controls), nerve hypoechogenicity in 86%, and focal lesions in 20%, according to a study by Powell et al. [54] (Fig. 8). Interestingly this nerve may be affected not only at the anterior superior iliac spine, but also at different levels along its course, where multiple US-guided injections might be recommended [55].
Peroneal Nerve
Peroneal neuropathy is the most common compressive neuropathy of the lower extremity. It should be included in the differential diagnosis for patients presenting with foot drop, pain of the lower extremity, or numbness of the lower extremity. Symptoms of peroneal neuropathy may occur due to compression of the common peroneal nerve (CPN), superficial peroneal nerve (SPN), or deep peroneal nerve (DPN), each with different clinical presentations. The CPN is most compressed at the level of the bony prominence of the fibular head, the SPN is most entrapped as it exits the lateral compartment of the leg, and the DPN as it crosses underneath the ankle extensor retinaculum [56-58].
The CPN arises from the sciatic nerve and is subject to a variety of abnormalities. Although the diagnosis is often based on clinical findings and electrodiagnostic tests, high-resolution US plays an increasingly important role in determining the type and location of CPN abnormalities [59].
US can demonstrate an increased CSA of the CPN and changes in nerve echotexture, including the loss of normal fascicular echotexture and an increased echogenic rim (Fig. 9) [60]. The normal mean CSA values at these anatomical sites were reported to be 13.2 mm2 at the fibular head and 11.4 mm2 at the fibular tunnel [61], whereas a CSA of 17.2 mm2 was considered pathological [62].
If the CSA is normal at the fibular head, a further more proximal examination towards the junction with the sciatic nerve should be performed.
MortonŌĆÖs Neuroma
According to a study by Quinn et al. [63], US can reveal Morton's neuroma in 85% of cases.
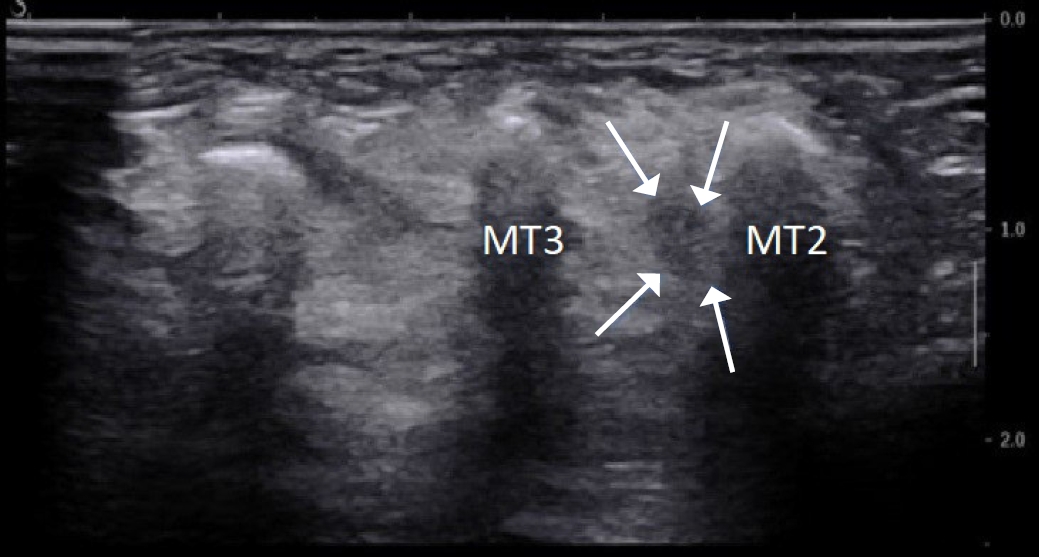
Morton's neuroma is a commonly encountered cause of forefoot pain, which may limit weight-bearing activities and footwear choices. Although the etiology and pathomechanism of this condition remain a matter of debate, the histological endpoint is well established as benign perineural fibrosis of a common plantar digital nerve, typically within the third intermetatarsal space. The most probable cause is a constriction at the level of the intermetatarsal ligament, which in most cases is caused by inappropriate weight put on the forefoot [48,64,65].
A recent study by Del Mar Ruiz-Herrera et al. [66] demonstrated an association between the occurrence of Morton┬┤s neuroma and a smaller space between the metatarsal heads of the third and the fourth metatarsals and under the deep transverse metatarsal ligament using US.
The diagnosis can be accomplished using US with a high level of accuracy and reproducibility [67,68]. The US findings include a reactive tissue mass with a spindle-like shape, presenting with decreased heterogeneous echogenicity and increased vascular flow. Morton's neuroma can be visualized by applying the transducer to the dorsal part of the foot, additionally pressing against the intermetatarsal space from the plantar part. This maneuver enables the movement of the neuroma in the dorsal direction (Fig. 10) [48,69]. Sonographic palpation is further useful when localizing MortonŌĆÖs neuromas, as they can also present variably at a more proximal level and at a dorsal or plantar location. Identification of the presumed plantar digital nerve in continuity with the mass improves diagnostic confidence. The long-axis view often allows the identification of continuity between the common plantar digital nerve and the neuroma. Detection of the plantar digital nerve entering the neuroma can raise the diagnostic accuracy for Morton's neuroma relative to other intermetatarsal masses, such as complicated ganglion cysts or tendon sheath fibromas [70,71].
Elastography
Although measuring the CSA values of the affected nerves is a good and well-established method, this parameter was also shown to suffer from a lack of standardization, which negatively affected its sensitivity and specificity [72,73]. Sonoelastography is a US imaging technique that allows a noninvasive estimation of tissue stiffness, which might add value to the diagnostic performance of US in entrapment neuropathies [74]. This technique is based on the fact that softer tissue exhibits greater tissue displacement than hard tissue when externally compressed. Entrapment neuropathies are associated with a significant increase in the stiffness of affected nerves, which can be accurately detected with US elastography [72]. Furthermore, Klauser et al. [75] showed that the perineural area, as in CTS, was stiffer in patients than in healthy volunteers.
Conclusion
High-resolution US is a feasible, fast, and reliable method to diagnose and monitor nerve entrapment syndromes and to guide diagnostic and therapeutic perineural injections. US findings include enlargement of the diameter and CSA of the nerve at the site of compression, hourglass narrowing in the longitudinal section, the loss of echotexture, echogenic perineural fibrosis, decreased mobility, and intraneural fibrosis in longstanding entrapment conditions.



 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI



