Ultrasonographic diagnosis of ovary-containing hernias of the canal of Nuck
Article information

Abstract
Purpose:
The purpose of this study is to describe the ultrasonographic findings of ovary-containing hernias of the canal of Nuck.
Methods:
This was a retrospective analysis of 22 hernia cases of the canal of Nuck. The following gray scale and color Doppler ultrasonographic features were analyzed: the site and the size of the hernia, the texture of the hernia contents, and the presence or absence of blood flow in the hernia contents.
Results:
All of the patients had swelling of the right inguinal region (n=10), left inguinal region (n=8), or both (n=2). On ultrasonography, the hernias appeared as either solid masses (n=17) or solid masses containing cysts (n=5). The mean anteroposterior diameter of the hernia sac of the canal of Nuck was 9.1 mm (range, 5 to 18 mm). The mean anteroposterior diameters of the hernia sac were 11.6 mm (range, 7.6 to 18 mm) for hernias containing an ovary, and 8.3 mm (range, 5 to 13 mm) for hernias containing omental fat. During surgery, among the 17 cases with solid-appearing hernia contents on ultrasonography, omental fat was identified in the hernia sac in four cases, but no structure was identified in 13 cases. All five cases that appeared as solid masses containing cysts on ultrasonography contained ovary tissue in the hernia sac. Among the four cases of ovary-containing hernias, color Doppler ultrasonography identified blood flow within the ovary in three cases, but no flow signal was seen in one case of incarcerated hernia.
Conclusion:
Ultrasonography may be helpful for the diagnosis of ovary-containing hernias of the canal of Nuck by detecting solid masses containing small cysts.
Introduction
In women, the round ligament is attached to the uterus near the origin of the fallopian tube, and a small evagination of parietal peritoneum accompanies the round ligament through the inguinal canal to the labium majorum. This small evagination of parietal peritoneum, named the canal of Nuck in women, is the equivalent of the processus vaginalis in men [1].
In the normally developing female fetus, the canal of Nuck is usually obliterated by 8 months of gestation. Failed complete obliteration of this structure results in an indirect inguinal hernia of the canal of Nuck [2]. In the case of a hernia of the canal of Nuck in female infants, early diagnosis is important when the hernia contains an ovary, because incarceration of the ovary is common and has been reported in up to 43% of cases [3]. Therefore, a female infant with an inguinal hernia should be evaluated to determine whether the ovarian contents are present.
Although several cases of ovary-containing hernias of the canal of Nuck have been reported, imaging findings have rarely been described [4-6]. In addition, although ultrasonography is the firstline diagnostic examination for the evaluation of inguinal lesions, sonographic descriptions of ovary-containing hernias of the canal of Nuck are scant. To the best of our knowledge, the ultrasonographic findings of ovary-containing hernias of the canal of Nuck have been presented in fewer than 20 cases [7-17]. The aim of this study was to evaluate the ultrasonographic findings of ovary-containing hernias of the canal of Nuck.
Materials and Methods
This retrospective review of sonographic studies was approved by the Institutional Review Board of our institution. Patients with surgically-confirmed hernias of the canal of Nuck were recruited at our institution between January 2007 and August 2013, and those who underwent ultrasonography before surgery were included. Preoperative physical examination findings were recorded.
All ultrasonographic examinations were performed with a 5-MHz to 12-MHz transducer and an IU 22 unit (Philips Medical Systems, Bothell, WA, USA). We routinely scanned both inguinal areas in transverse and longitudinal planes. Color Doppler ultrasonography was performed with optimized color Doppler parameters. The power level, threshold, persistence, and wall filter were individually adjusted to maximize the detection of blood flow through the field of view.
Ultrasonographic findings were determined by retrospective analysis of images. Three radiologists (DMY, HCK, and SWK) interpreted the gray scale and color Doppler ultrasonograms. The site and the size of the hernia, the texture of the hernia contents, and the presence or absence of blood flow through the hernia contents were determined by three radiologists working in consensus. In terms of the texture of the hernia contents, we classified it into a solid mass or solid mass containing cysts. The term “solid mass” refers to any non-cystic lesion on ultrasonography. The echogenicity of the solid mass was divided into isoechoic or hypoechoic compared with adjacent inguinal fatty tissue. Measurement of the hernia sac was performed in the maximal anteroposterior diameter.
We performed a statistical analysis to compare the size of the hernia sacs containing an ovary with the size of hernia sacs containing other structures using Wilcoxon rank sum test. Probability values less than 0.05 were considered statistically significant. The data were analyzed using a SPSS ver. 18 (SPSS Inc., Chicago, IL, USA).
Results
Twenty-two hernias of the canal of Nuck in 20 patients were included. Two patients had bilateral hernias of the canal of Nuck. The patients ranged in age from 1 month to 137 months (mean age, 51 months). All of the patients had swelling of the right inguinal region (n=10), left inguinal region (n=8), or both (n=2). All of the patients were medically well before admission and had no history of prior abdominal surgery.
All patients underwent complete ultrasonography before surgery. The duration between ultrasonography and surgery was 7 days on average (range, 0 to 25 days). The correlation between ultrasonography and the surgical findings in 22 cases of hernia of the canal of Nuck is summarized in Table 1. On ultrasonography, the hernia contents appeared as solid masses (n=17) (Fig. 1) or solid masses containing cysts (n=5) (Figs. 2-4). The echogenicity of the solid mass was isoechoic to the inguinal fat (n=17) and hypoechoic in solid masses containing cysts (n=5). In surgery, among the 17 cases with a solid appearance of the hernia contents on ultrasonography, omental fat was identified in the hernia sac in 4 cases (Fig. 1), but no structure was identified in 13 cases. All 5 cases that appeared as solid masses containing cysts on ultrasonography contained ovary tissue in the hernia sac.
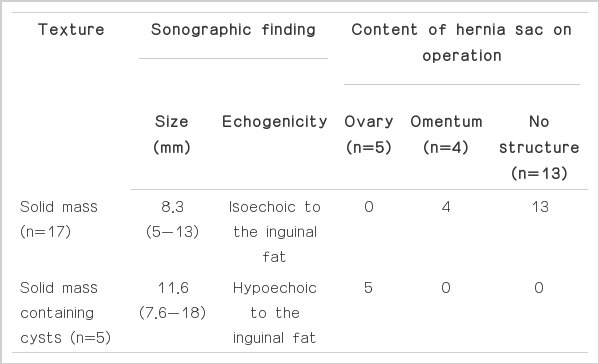
Correlation of sonographic and surgical findings for 22 cases of hernia of the canal of Nuck
Omental fat-containing hernia of the canal of Nuck in a 45-month-old girl.
Longitudinal gray scale ultrasonography shows an ovoid, heterogeneously hyperechoic, solid mass in the right inguinal area (arrow), which was found to be omental fat on operation.

Ovary-containing hernia of the canal of Nuck in a 3-month-old girl.
A. Longitudinal gray scale ultrasonography shows an ovoid, solid mass containing cysts in the right inguinal area (arrow). B. On color Doppler ultrasonography, blood flow is seen in the mass (arrow).
Ovary-containing hernia of the canal of Nuck in a 1-month-old girl.
A. Longitudinal gray scale ultrasonography shows an ovoid, solid mass containing cysts in the right inguinal area (arrow), which extends to the abdominal cavity through the neck of the canal of Nuck (thin arrows). B. On color Doppler ultrasonography, blood flow is seen in the mass (arrow).
An incarcerated ovary-containing hernia of the canal of Nuck in a 4-month-old girl.
A. Longitudinal gray scale ultrasonography shows an ovoid, hypoechoic mass with internal tiny cysts (arrow). B. Longitudinal color Doppler ultrasonography shows no blood flow within the mass (arrow). C. Photomicrography shows hemorrhagic necrosis of the ovary. Hemorrhagic necrosis of the peripheral follicles is seen (arrows) (H&E, ×20).
The mean anteroposterior diameter of the hernia sac of the canal of Nuck was 9.1 mm (range, 5 to 18 mm). The mean anteroposterior diameters of the hernia sac were 11.6 mm (range, 7.6 to 18 mm) for hernias containing an ovary, and 8.3 mm (range, 5 to 13 mm) for hernias containing omental fat. The mean size of the hernia sac containing an ovary was larger than for those containing omental fat, but there was no statistically significant difference between the two groups (P>0.05).
Among the five cases of an ovary-containing hernia, color Doppler ultrasonography was performed in four cases. On color Doppler ultrasonography, the blood flow was identified within the ovary in three cases, but no flow signal was seen in one. In one case of incarcerated hernia (Fig. 4), the ovary was found to have undergone torsion at the time of operation. The strangulated ovary was enlarged, with lower echogenicity compared with inguinal fat, and contained small cysts on gray scale ultrasonography. In our study, one of five cases with an ovary-containing hernia had strangulation of the ovary. The ovary was black and necrotic. Oophorectomy was performed. Gross and microscopic examination revealed a hemorrhagic necrotic right ovary (Fig. 4C).
Discussion
For hernias of the canal of Nuck, the peritoneal contents, including the bowel, omentum, fluid, and urinary bladder, can herniate into the inguinal canal. In female patients, the sliding inguinal hernia contains the ovary with or without the Fallopian tube in 15% to 20% of cases [8]. In our study, five of 22 cases (23%) were ovarycontaining hernias of the canal of Nuck.
Although ovary-containing hernias of the canal of Nuck can be discovered at any age, they are most common in children. In one study, 71% of cases of inguinal hernias of the adnexa occurred in children younger than 5 years, and 29% occurred in adolescents or women of reproductive age [18]. In our study, all of the patients were children, ranging in age from 1 month to 137 months.
In most of the reported cases, the size of the hernia of the canal of Nuck is less than 3 cm. The hernia’s small size in women compared to men may be due to the smaller size of the female processus vaginalis than its male counterpart. In our study, the mean anteroposterior diameter of the hernia sac of the canal of Nuck was 9.1 mm (range, 5 to 18 mm). The mean size of the hernia sac was larger in cases of hernias containing an ovary than in those containing omental fat, but there was no statistically significant difference between the two groups (P>0.05).
Inguinal hernias are more common on the right side, occurring in approximately 60% of cases, with 30% on the left side, and 10% bilateral [19]. In our study, the right side (55%) was more common.
Ultrasonography is an easily applied and highly accurate imaging modality. Ultrasonography with a high-frequency transducer is the imaging modality of choice for evaluating the inguinal lesion. It provides excellent spatial resolution and assists in the identification and characterization of inguinal lesions [20]. In the characterization of the hernia contents, the visualization of ovary-like structures containing peripheral cysts on ultrasonography was helpful for the diagnosis of the hernia contents as ovary tissue [12,13]. In our study, all five hernias containing ovaries appeared as solid masses containing small cysts on ultrasonography. The small cystic lesions presented as ovarian follicles on pathologic correlation. We believe that the ultrasonographic finding of solid masses containing multiple cysts of varying size is a useful sign for the identification of ovarycontaining hernias.
Early diagnosis is important when the hernia contains an ovary, because incarceration of the ovary is common [3]. Incarcerated ovaries in infants are at risk of torsion. If torsion of the ovary occurs, the venous and lymphatic return of the ovary within the canal of Nuck is impaired, causing increased swelling and pressure. This is usually accompanied by symptoms such as severe irritability, abdominal pain, and vomiting. Gangrene and tissue necrosis of the ovary supervene if the hernia is not reduced [21]. Ultrasonographic findings of ovary torsion are an enlarged, mass-like ovary with heterogeneous echogenicity that contains multiple peripheral cysts and no blood flow within the ovary [22].
In our study, one of five cases with an ovary-containing hernia had strangulation of the ovary. The strangulated ovary was enlarged, with lower echogenicity compared with inguinal fat, and contained small cysts on gray scale ultrasonography with no blood flow within the ovary on color Doppler ultrasonography. The herniated ovary showed infarction due to incarceration. Gross and microscopic examination revealed a hemorrhagic necrotic right ovary, including follicles.
Interestingly, 13 of 17 cases with solid-appearing hernia contents on ultrasonography did not have any structure in the hernia sac on operation. We think that the hernia contents had spontaneously reduced through the internal inguinal ring before surgery, either during anesthesia induction or during groin dissection. We propose that the contents of the hernia sac in all of these 13 cases were most likely omental fat because they showed a solid echo texture without internal cystic portions.
Our study was limited by its small study population, and all of the patients were children. Therefore, further studies with large sample sizes are necessary to examine the ultrasonographic findings of hernias of the canal of Nuck that contain ovary tissue. Despite these limitations, familiarity with the ultrasonographic findings of hernias of the canal of Nuck that contain ovary tissue is important for the diagnosis of patients with an inguinal mass.
In conclusion, an ovary-containing hernia of the canal of Nuck is a rare type of inguinal mass. Ultrasonography may be helpful for the diagnosis of ovary-containing hernias of the canal of Nuck by detection of solid masses containing small cysts. Even without signs of strangulation, hernias containing ovaries should be managed with early surgical reduction after the detection of an ovary within the hernia sac.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This study was supported in part by the Research Fund of the Korean Society of Ultrasound in Medicine.