

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Thyroid nodules are common, with an incidental detection rate of 19% to 68% [1-4]. Fine needle aspiration biopsy (FNAB) is an optimal diagnostic tool for thyroid nodules because it is cost-effective, safe, and accurate [5-8]. While the Bethesda guidelines for thyroid FNAB recommend that the unsatisfactory rate on cytopathology should be approximately 10% [9], the unsatisfactory rate ranges from 0.4% to 40.7% depending on the operatorŌĆÖs experience [10]. For that reason, recent studies have reported the utilization of first-line or second-line core needle biopsy to increase diagnostic yield [11-13].
The conventional to-and-fro technique for FNAB may be suboptimal for effective and safe specimen acquisition. To-andfro movement while visualizing the needle tip and simultaneously applying negative pressure can be challenging when the nodule is small, ill-defined, or located near anatomical structures like major vessels, the trachea, and the esophagus. Furthermore, poor cooperation by the patient, such as coughing, swallowing, talking, or making inappropriate jaw motion, can obscure the visualization of the needle tip to a great extent. More importantly, intranodular hemorrhage due to the repetitive to-and-fro motion combined with forceful aspiration can contaminate the specimen with blood [2,14]. Furthermore, failure of constant needle tip visualization during procedure can cause injuries to major vessels, the trachea, the esophagus, or nerves, which may necessitate more aggressive management than icepack application or manual compression [15].
Herein, we devised a novel whirling FNAB technique that may help harvest specimens effectively and safely by ensuring needle tip visualization, especially in difficult biopsy situations. The purpose of this study was to compare thyroid FNAB techniques (conventional to-and-fro vs. whirling) in terms of cell harvesting ability ex vivo, the unsatisfactory rate and complication rate in vivo, and multioperator performance in phantom models simulating difficult biopsy situations.
Materials and Methods
Conventional FNAB Technique
The conventional FNAB technique was performed under ultrasonography guidance (Canon Medical Systems Co., Seoul, Korea), using a 7.5-14 MHz linear probe and a 24-G needle with a 10-mL syringe in a parallel orientation [16]. The transisthmus needle approach was implemented. As the needle tip was visualized at the very surface of the thyroid, the needle was advanced slowly until the needle tip was placed at the target. The specimen was collected with six to seven to-and-fro motions for 10 seconds to induce capillary sampling [10]. In order to further facilitate capillary sampling, a slight negative pressure was created with regular aspiration of 3 mL during the to-and-fro motion [10]. If an insufficient amount of specimen was visualized at the needle hub, we repeated the to-and-fro motion at different quadrants of the nodule by tilting the needle angle or by relocating the needle tip [10,17]. We released the negative pressure before withdrawing the needle to prevent needle tract seeding or hemorrhage [10,15]. We performed only one conventional FNAB in each session.
Whirling FNAB Technique
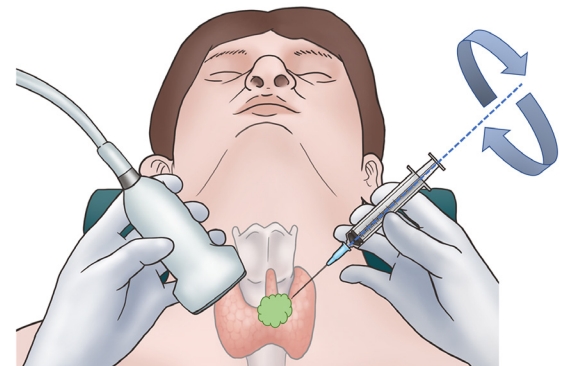
The whirling FNAB technique was performed under the same settings as the conventional FNAB technique. When the needle tip was visualized at the target, the operator alternately rotated the needle back and forth (i.e., made a whirling motion) with the index finger and third finger, while the thumb served as a fulcrum (Fig. 1). The fourth finger and fifth finger were placed on the syringe for additional stability during tissue sampling. The whirling motion was applied gently 10 to 15 times for 10 seconds. The application and release of a slight negative pressure, as well as the strategy for an insufficient amount of the specimen, were the same as in the conventional FNAB technique. We performed only one whirling FNAB in each session.
Ex Vivo Study
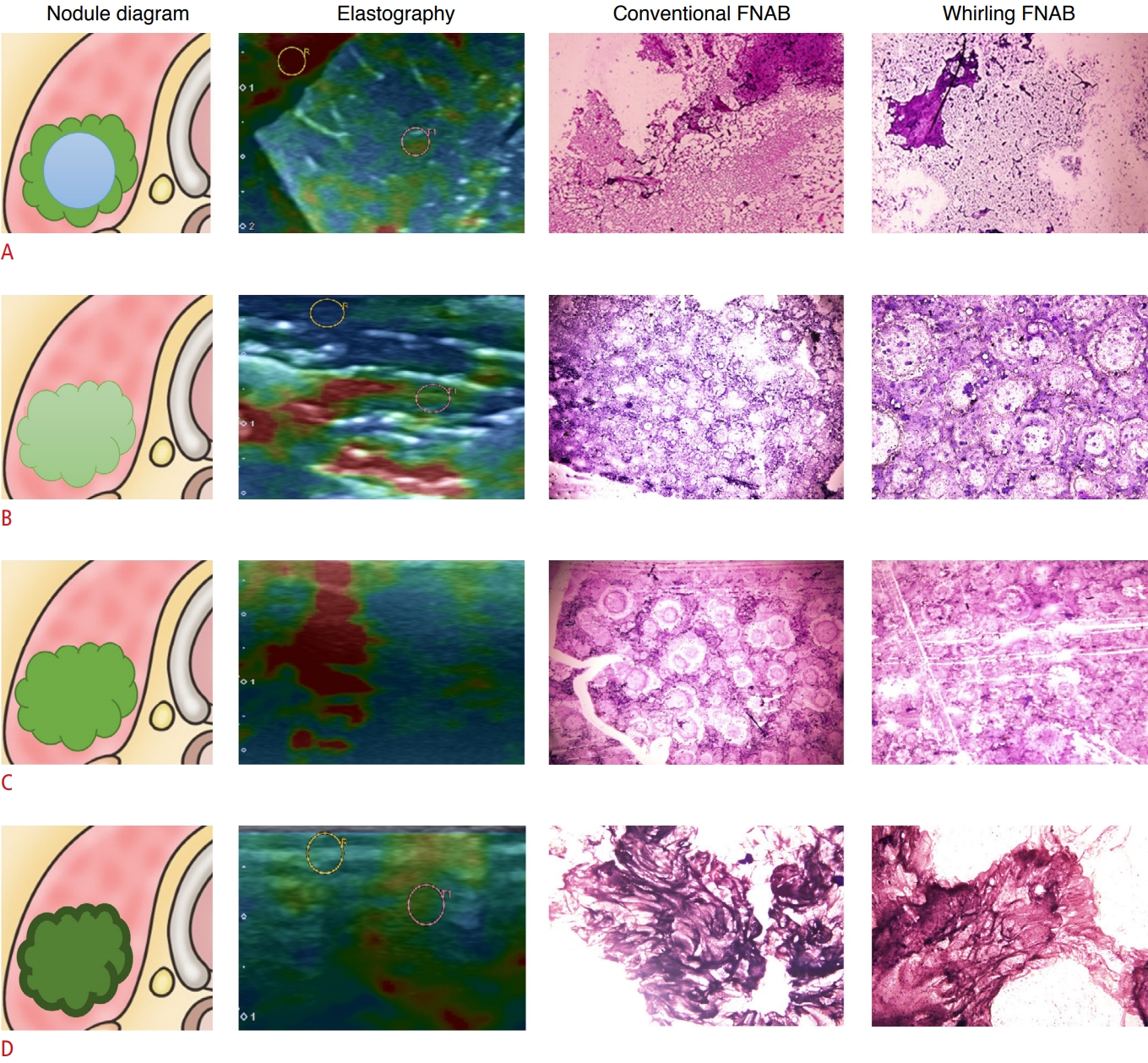
Under institutional review board (IRB) approval, an ex vivo study was conducted using commercially available orange pulp and bovine tissues, which did not include any experimentation on live animals or extraction of tissues from live animals. Orange pulp suspended in sweet jelly, bovine liver, bovine lung, and bovine muscles from the anterior part of thigh were utilized. Strain elastography was performed on each specimen to measure strain values. The orange pulp simulated a cystic thyroid nodule, while the bovine lung, bovine liver, and bovine muscle simulated solid thyroid nodules with various elasticity values. Two board-certified radiologists (the first radiologist with more than 10 years of experience in thyroid imaging, and the second radiologist with 2 years of experience in thyroid imaging and thyroid interventions) performed the FNABs. Both the whirling technique and conventional to-and-fro technique were applied twice for each thyroid nodule mimicker for less than 20 seconds to simulate in vivo FNAB. Each harvested specimen was smeared on a slide using 95% ethyl alcohol, fixed, and stained with azure-eosin-methylene blue (Giemsa solution, Sigma-Aldrich, Seoul, Korea). To measure cell harvesting ability, cell counts per background at ├Ś100 magnification were semi-quantitatively recorded for each slide and the median values were compared (Fig. 2). Referring to the 2017 Bethesda system for cytology [18], specimens with fluid only, acellular specimens, blood-contaminated specimens, and thick smears were defined as unsatisfactory.
In Vivo Study
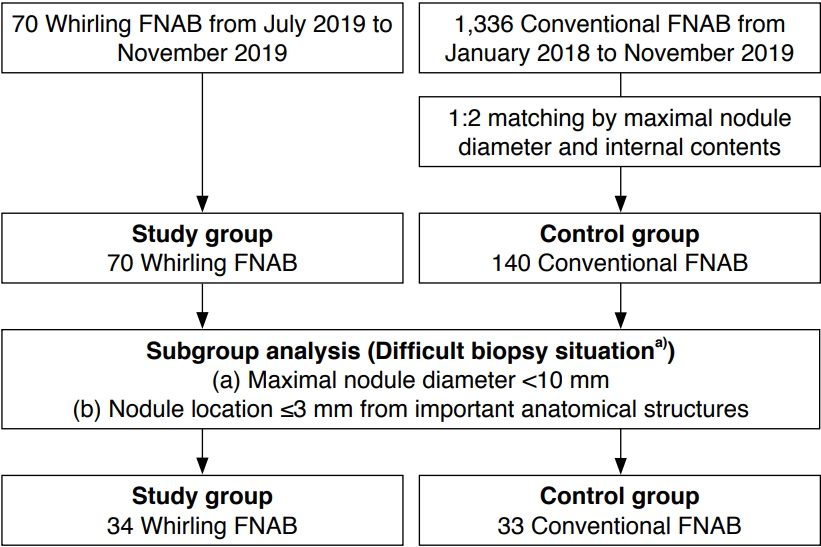
Our IRB approved the retrospective review of the medical records and images of patients who underwent thyroid FNAB at our institution from January 2018 to November 2019 with a waiver of informed consent from patients (Fig. 3).
The same two board-certified radiologists (the first radiologist with 10 years of experience in thyroid imaging, and the second radiologist with 2 years of experience in thyroid imaging and thyroid interventions) routinely classified the thyroid nodules based on ultrasonography findings according to the Korean Thyroid Imaging Reporting and Data System (K-TIRADS) as follows: category 1, no nodule; category 2, benign nodule; category 3, nodule with low suspicion; category 4, nodule with intermediate suspicion; and category 5, nodule with high suspicion of malignancy [19]. Our institutional indications for thyroid FNAB were in compliance with the revised Korean Society of Thyroid Radiology guideline published in 2016 [3,19]. Any solid hypoechoic nodules greater than 10 mm with suspicious features such as microcalcification, non-parallel orientation, and spiculated or microlobulated margins were indications for FNAB. Based on the discretion of the referring physicians and shared decision-making, any solid hypoechoic nodules less than 10 mm with suspicious ultrasonographic features with or without a family history of thyroid cancer, growth tendency, and radiation history were indications for FNAB. Specimens were either prepared on a slide using 95% ethyl alcohol or in alcohol-based solutions for liquid-based cytology by a dedicated technician in the radiology department. According to the Bethesda system [18], specimens were interpreted by one of five boardcertified pathologists with at least 2 years of experience in thyroid cytopathology.
The novel whirling FNAB technique was performed in 70 randomly selected patients (i.e., the study group) from July 2019 to November 2019 by the second board-certified radiologist with 2 years of experience in thyroid imaging and interventions. For the control group, 1,36 patients were enrolled who underwent conventional thyroid FNAB from January 2018 to November 2019 performed by one of the three radiologists (the same two radiologists who performed the ex-vivo FNABs and another radiologist with 10 years of experience in thyroid imaging). A further selection was made by 1:2 nearest matching to the study group based on the maximal nodule diameter and the internal content of the nodule. The FNAB for the control group was performed by one of two board-certified radiologists. Age, sex, nodule content, calcification, intranodular vascularity, nodule diameter, K-TIRADS category, specimen preparation, pathologic results, the unsatisfactory rate, and the complication rate were retrospectively reviewed for the study group and control group. In accordance with the Society of Interventional Radiology and other studies, major complications were defined as follows: permanent adverse sequelae, complications requiring surgical intervention, and/or complications requiring hospitalization [20-22]. We evaluated the effectiveness of each FNAB technique by assessing the unsatisfactory rate and safety by assessing the complication rate.
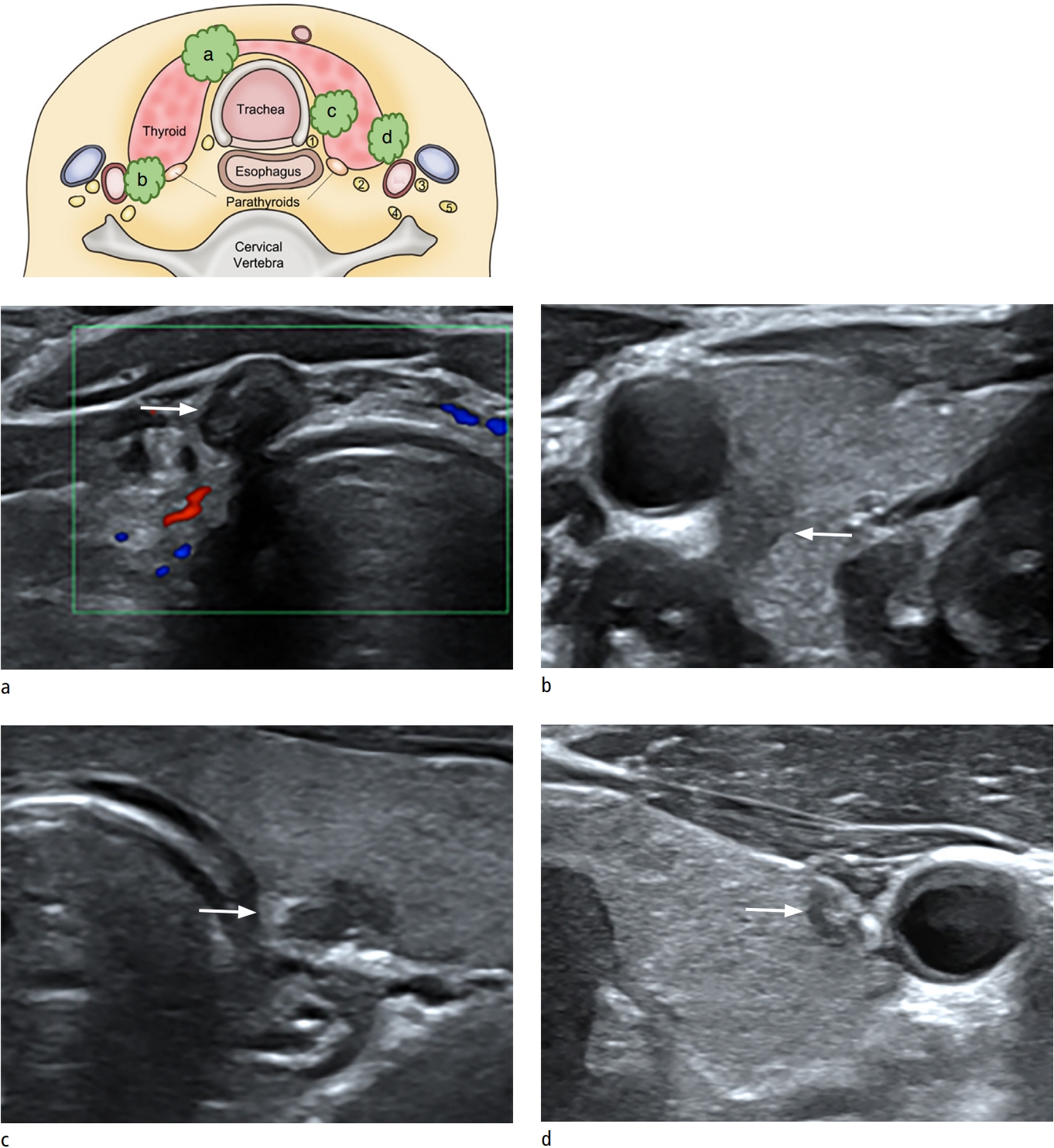
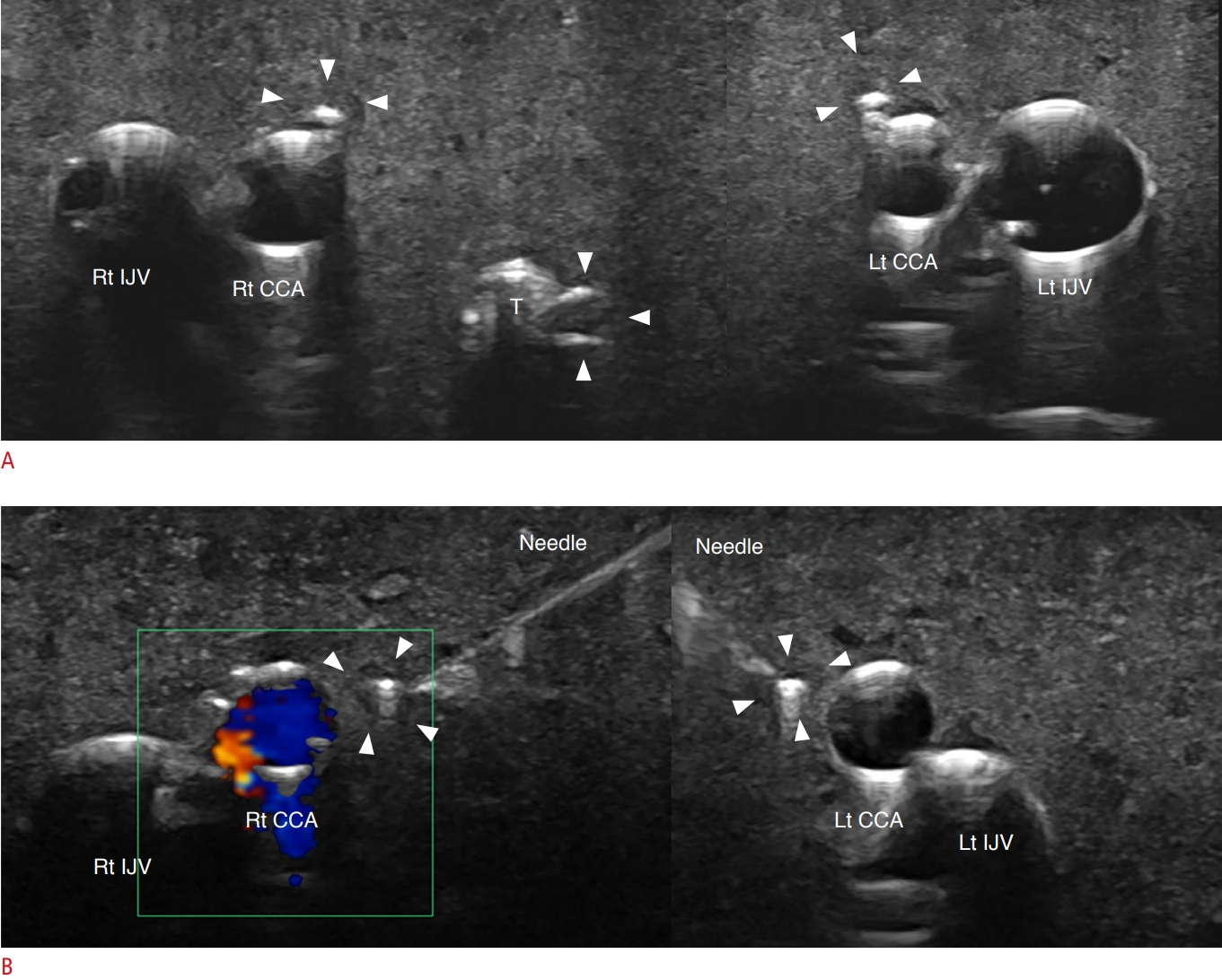
We also evaluated how these techniques performed in difficult biopsy situations in terms of the unsatisfactory rate and complication rate. We defined and subcategorized difficult biopsy situations for each technique as follows: a thyroid nodule with a maximal diameter less than 10 mm and located within 3 mm of anatomical structures such as the common carotid artery, esophagus, trachea, and perithyroidal vessels (Fig. 4). Any thyroid nodules larger than 10 mm and located more than 3 mm away from anatomical structures were excluded.
Phantom Study
The phantom study was designed to simulate difficult biopsy situations in real clinical settings. Thyroid phantom models were created utilizing commercially available tofu (bean curd), commercially available straws, and 24-gauge needles, as proposed by Zhang et al. [23]. An empty 2-mL syringe was inserted at the midline of the tofu to simulate the phantomŌĆÖs trachea, and small- and large-caliber straws filled with ultrasonography gel were inserted at each edge of the tofu to simulate common carotid arteries and internal jugular veins, respectively. Manual pumping was applied to 30-mL syringes filled with water and connected to the phantom arteries by a study coordinator to mimic arterial pulsations. Phantom thyroid nodules smaller than 10 mm were simulated with 24-gauge needles and inserted at locations within 3 mm of the phantom trachea and phantom vessels (Fig. 5).
Eight operators with various levels of experience in thyroid FNAB (novice operators, two second-year radiology residents and two third-year radiology residents; experienced operators, two fourth-year radiology residents and two board-certified radiologists) participated in the phantom study. A study coordinator instructed the operators regarding the techniques prior to the experimental session, and a practice session was provided to the operators over the course of a week. Each operator performed both techniques for two phantom nodules. The study coordinator judged the adequacy of each FNAB by each operator using the following criteria: (1) correct targeting, (2), correct needle trajectory, (3) avoidance of phantom trachea and vessels, and (4) correct to-and-fro movement or whirling motion. After the experimental session, operators responded to questionnaires evaluating their level of dexterity, level of needle tip visualization, and preference using a 5-point Likert scale (1, strongly disagree; 2, disagree; 3, neither agree nor disagree; 4, agree; 5, strongly agree).
Statistical Analysis
For the ex vivo study, cell harvesting abilities were compared between the two techniques using the Mann-Whitney U test. For the in vivo study, the control group was selected by using nearest matching to the study group with a 1:2 ratio based on the maximal diameter and internal content of nodules. The Student t-test or the Mann-Whitney U test was performed to compare continuous variables, and the chi-square test was used to compare categorical variables in the ex vivo study and phantom study. The R statistical program (version 3.6.1, The R Foundation for Statistical Computing, Vienna, Austria) was used for the analysis. A two-sided P-value less than 0.05 was considered to indicate statistical significance.
Results
Ex Vivo Study
The strain values measured for the orange pulp, bovine liver, bovine lung, and bovine muscle were 0.02%, 0.3%, 0.4%, and 8.4%, respectively. Thus, the orange pulp, bovine liver or lung, and bovine muscle represented tissue with high, medium, and low elasticity, respectively, and were considered to mimic thyroid nodules with various elasticity values (Fig. 4). The cell harvesting ability was comparable between conventional FNAB and whirling FNAB (median semiquantitative cell counts per background on ├Ś100 magnification microscope field: conventional technique, 80.0% vs. whirling technique, 87.5%, P=0.178). No unsatisfactory specimens were obtained using either technique.
In Vivo Study
The mean patient age (58.5┬▒11.8 years vs. 57.6┬▒13.4 years, P=0.981) and the proportion of women (87.1% vs. 87.1%, P=0.990) were comparable between the control group and the study group (Table 1). The nodule content (solid, predominantly solid, predominantly cystic) was comparable between both groups (P=0.434). Calcification (none, microcalcification, rim calcification, or macrocalcification) was also comparable between both groups (P=0.572). Additionally, the Doppler signals representing intranodular hypervascularity (none or minimal, perinodular hypervascularity, and hypervascularity) were comparable between both groups (P=0.413). The mean nodule diameter was smaller in the study group than in the control group (anterior to posterior, 9.2┬▒5.2 mm vs. 8.8┬▒6.0 mm; width, 12.2┬▒7.6 mm vs. 7.5┬▒5.0 mm; caudal to cranial, 15.5┬▒9.8 mm vs. 8.6┬▒6.9 mm; P<0.001 for both groups). The K-TIRADS category (P=0.054) and the method of specimen preparation were comparable between the techniques (P=0.144). The Bethesda category (P=0.859) was also comparable between the techniques. The unsatisfactory rate was 15.7% and 12.9% in the control group and study group, respectively (P=0.859). Two minor complications occurred in the control group: puncture at the right common carotid artery and subcutaneous hematoma at the puncture site (1.4% vs. 0%, P=0.553) (Table 1). These complications were managed with manual compression and application of an icebag. No hospitalization nor surgical interventions were required for these two patients and no permanent adverse sequelae were observed.
When we conducted a subanalysis of difficult biopsy situations (thyroid nodule <10 mm and located within 3 mm of major anatomical structures), 33 thyroid nodules were considered to represent difficult situations for the to-and-fro conventional technique and 34 thyroid nodules were considered to represent difficult situations for the whirling technique. Within the subgroup of difficult biopsy situations, the conventional technique group had eight unsatisfactory cases (24.2%) and two cases of complications (6.1%), while the whirling technique group had only two unsatisfactory cases (5.9%) and 0 complications. In difficult biopsy situations, the whirling technique demonstrated a lower unsatisfactory rate than the conventional technique (24.2% vs. 5.9%, P=0.045). Although two cases of complications (common carotid artery puncture and subcutaneous hematoma) occurred in the conventional group, the difference in the complication rate between the groups was not statistically significant (6.1% vs. 0%, P=0.239).
As summarized in Table 2, within the subgroup of non-difficult biopsy situations, the conventional technique group had 14 unsatisfactory cases (13.1%) and no complications, while the whirling technique group had seven unsatisfactory cases (19.4%) and no complications. In non-difficult biopsy situations, the whirling technique and the conventional technique were comparable in terms of the unsatisfactory rate (13.1% vs.19.4%, P=0.351) (Table 2).
Phantom Study
The adequacy criteria were satisfied for both techniques by all operators. Although novice operators required additional instructions and practice time, they successfully performed both techniques without any failed attempts.
As summarized in Table 3, all operators reported that the whirling technique was easier to perform, easier to control, easier for visualization of the needle tip, and preferable to the conventional technique in simulated difficult biopsy situations. The median scores for the level of dexterity were 1.5 (interquartile range [IQR], 1 to 2) for the conventional technique and 4 (IQR, 4 to 4.25) for the whirling technique (P<0.001). The median scores for the level of needle tip visualization were 2 (IQR, 2 to 3) for the conventional technique and 4 (IQR, 3.75 to 4.25) for the whirling technique (P=0.002). The median score for preference of the whirling technique was 4 (IQR, 4 to 4.25) (Table 3).
There were no significant differences in the median scores between novice operators and experienced operators for both techniques: level of dexterity for the conventional technique, 1 (IQR, 1 to 1.25) vs. 2 (IQR, 1.75 to 2.25), P=0.065; level of dexterity for the whirling technique: 4 (IQR, 3.75 to 4.25) vs. 4 (IQR, 4 to 4.25), P=0.574; level of needle tip visualization for the conventional technique: 2 (IQR, 2 to 2.25) vs. 2.5 (IQR, 1.75 to 3), P=0.878; level of needle tip visualization for the whirling technique: 4 (IQR, 3.75 to 4.25) vs. 4 (IQR, 3.75 to 4.25), P>0.99; and preference for the whirling technique: 4 (IQR, 4 to 4) vs. 4.5 (IQR, 4 to 5), P=0.105.
Discussion
Our study results demonstrate that the novel whirling technique is feasible and may be effective and safe for thyroid FNAB. The ex vivo comparison showed that cell harvesting was successful using both techniques for all thyroid nodule mimickers. The in vivo study showed that both techniques demonstrated acceptable unsatisfactory rates, near 10%, as recommended by the Bethesda guidelines [9]. In difficult biopsy situations, the whirling technique demonstrated better performance than the to-and-fro conventional FNAB technique, with a lower unsatisfactory rate and lower complication incidence. In the phantom study, despite differences in operatorsŌĆÖ FNAB experience levels, it was found that the whirling technique might be easier to perform, easier to visualize (and easier to control), and more preferable than the conventional technique in simulated difficult biopsy situations.
Several previous studies have investigated the optimal techniques for thyroid FNAB. Titton et al. [24] and Oertel [25] recommended that applying negative pressure is not necessary unless capillary sampling is not spontaneously attained. This "combined method" involving negative pressure was reported to result in the harvest of sufficient specimens and a reduction of procedure-related complications [10]. Another study showed that FNAB could even be performed without applying negative pressure [26]. While both techniques used in our study were based on the combined method, the results of our study expand prior knowledge by showing that the novel whirling technique may be comparably effective and safe to the conventional to-and-fro technique. Furthermore, in difficult biopsy situations, the whirling technique may be more effective and safer than the conventional technique.
As assessed in the phantom study, the whirling technique enables constant needle tip visualization by fixing the needle tip in the same location. This constant needle tip visualization provides better control of the needle, which can reduce the unsatisfactory rate and the complication rate. In contrast, the conventional technique requires repeated advancement and retrieval of the needle along the axis, making constant visualization of the needle tip challenging. Therefore, the safety margin between a thyroid nodule and adjacent major anatomical structures is smaller in the conventional technique than in the whirling technique. Although the complication rate did not show a significant difference between the two techniques, and the two complications might have caused by the needle puncture rather than needle motion, the whirling technique may be preferable to prevent further complications in difficult biopsy situations, especially for novice operators.
We speculate that the driving biomechanical force for capillary sampling in the whirling technique is the outward force (i.e., the "centrifugal force") created by the rotating motion along the axis and the pressure gradient created by gentle aspiration. The centrifugal force is the force vector perpendicular to the axis of rotating motion exerted on the thyroid nodule that pulls tissue, fluid, and cells into the syringe. A recent article demonstrated that the centrifugal force is important in pulling on the dense solid-liquid phase field in a rotating channel [27], which is analogous to the thyroid nodule tissue pulled into the syringe during whirling FNAB. The article also showed that the centrifugal force depends on both the angular rotation speed and the concentration gradient across the channel. Therefore, proper execution of the rapid whirling motion may be essential for the whirling FNAB technique.
Our study has several limitations. First, the strain values measured in ex vivo experiments not be precisely the same as those measured in human thyroid nodules. However, we tried to implement the novel technique in thyroid nodule mimickers with various elasticities to represent various thyroid nodule contents in humans. Second, as the in vivo study only included a small number of predominantly cystic nodules, the effectiveness and safety of the whirling FNAB technique may be uncertain for predominantly cystic nodules. Nonetheless, the results using orange pulp in the ex vivo experiment may have implications for predominantly cystic nodules. Third, the whirling technique cannot be generalized to other operators since only one operator performed it in vivo. However, as the phantom study demonstrated, the whirling technique might be easy to learn and easy to perform, even for novice operators. Further studies measuring the needle tip visualization score and recruiting more operators with various levels of experience are warranted to strengthen the results of our in vivo study and phantom study. Lastly, due to the small sample sizes in the in vivo and ex vivo studies, there may have been selection bias in our study, and the subcategorization resulted in a much higher number of difficult situations in the whirling FNAB group. For the same reason, the unsatisfactory FNAB rate appeared higher (19.4%) in non-difficult biopsy situations for the whirling technique, although this difference was statistically insignificant compared to the conventional technique (15.7% vs. 19.4%, P=0.351). Nevertheless, we demonstrated that the whirling FNAB technique can be useful in difficult biopsy situations and that it may be a potential alternative technique when the conventional to-and-fro technique seems suboptimal. In order to further strengthen the evidence on the effectiveness and safety of the whirling technique, a prospective study with a large sample size, preferably a multi-center study, is necessary.
In the ex vivo study, both techniques demonstrated comparable and sufficient cell harvesting abilities. In the in vivo study, both techniques demonstrated comparable unsatisfactory and complication rates. In the subgroup analysis of difficult biopsy situations, the whirling technique performed better and had a lower unsatisfactory rate. In a phantom study, the whirling technique showed better dexterity and needle tip visualization, and was preferred to the conventional technique by all operators. The newly proposed whirling technique for thyroid FNAB may be effective and safe, especially in difficult biopsy situations, and it can be an alternative to the conventional to-and-fro technique.
 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



