

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Thyroid nodules are a very common occurrence in the general population, with a prevalence ranging between 20% and 76% [1]. The vast majority of thyroid nodules are benign and incidentally detected. Thyroid cancer is relatively uncommon, accounting for approximately 1%-5% of all cancers in females and fewer than 2% in males [2]. Benign thyroid nodules generally do not require any treatment, unless discomfort, dyspnoea, and hoarseness are present, when nodules present cosmetic concerns [3,4], or in cases of hyperfunctioning nodules [5]. The standard treatment of benign thyroid nodules still remains surgical resection [4,6]; however, this is a major surgical procedure, requiring general anaesthesia and hospitalization, with the complication rate ranging from 2.5% to 8.1% [7]. Further, skin scarring around the neck may be an undesired result of this type of surgery. In these cases, image-guided thermal ablation (IGTA) has been successfully used to achieve volumetric nodule reduction and symptom improvement [8-11]. IGTA is minimally invasive and has been reported to have good clinical results, thus indicating its potential to replace surgery as the first-choice treatment for benign thyroid nodules [12]. Moreover, IGTA techniques have been used in limited series for the treatment of malignant thyroid cancers, and in cases of recurrence after surgical excision of a primary cancer [13-19]. In this setting, IGTA still plays a limited role, but it represents a fascinating additional treatment within a multidisciplinary approach to thyroid cancer. Recently, new guidelines have been released by the Korean Society of Thyroid Radiology, including suggestions on indications for radiofrequency ablation (RFA) for benign and recurrent cancers [20]. This paper includes the most recent and authoritative indications and guidelines on the topic of IGTA in thyroid disease, which can also be applied to other modalities than RFA. Notably, as several other IGTA techniques have been applied in the treatment of thyroid diseases [11], and different specialists (radiologists, surgeons, endocrinologists) are currently performing IGTA, a more homogeneous standardization of indications, techniques, and even reporting criteria would be useful [21].
Percutaneous laser ablation (LA) was one of the first techniques used to perform IGTA, and is currently used in several different clinical scenarios, where its low invasiveness and high precision might offer clinical advantages over other ablative techniques [22-25]. LA was also one of the first techniques used for thyroid thermal ablation, and its use has been reported in the treatment of benign, hyperfunctioning, and malignant thyroid diseases [24,26-30]. In this paper, we review the application of LA in the thyroid, discussing its main clinical applications, results, and limitations.
LA Technique
The term "laser" originated as an acronym for "light amplification by stimulated emission of radiation." Laser light is highly coherent, collimated, and monochromatic, and can be precisely focused to deliver a high amount of energy to a very small area [31]. Laser light can be vehiculated from the source to a different point through an optical fibre, which can be designed according to the desired final energy delivery in terms of material, length, and tip shape [32,33]. When interacting with biological tissues, laser light undergoes scattering and is absorbed by tissues, with consequent deposition of energy and a controlled local increase in temperature [34].
Different laser sources (such as diodes or neodymium-yttrium aluminium garnet) and wavelengths can be used for clinical applications. For human therapies, the 1,064 nm wavelength seem to be ideal because of its properties in terms of tissue penetration and absorption. Thermal increases in temperature can cause tissue destruction by means of various mechanisms, including tissue carbonization and coagulative necrosis [35,36]. Irreversible cellular damage requires temperature exposure for a certain amount of time; it generally begins at a temperature of 46℃ when cells are exposed for about 60 minutes. At temperatures between 60℃ and 100℃, fast and permanent protein coagulation takes place, while temperatures over 105℃-110℃ induce tissue carbonization and vaporization [36-38].
Procedure
For the treatment of benign thyroid nodules with LA, the patient is placed on the operating table in the supine position with a hyperextended neck, peripheral venous access is obtained, and vital parameters are monitored.
Before treatment, the size, shape, and vascularization of the thyroid nodule are assessed using ultrasound. This preliminary evaluation needs to plan the number of fibers to use, the preferred access route, and the number of illuminations needed, according to nodule volume. A needle path as parallel as possible to the longest axis of the nodule is preferred. The procedure is performed using commercial ultrasound systems and a high-frequency linear transducer. A needle-guided attachment with adjustable angle selection can be used to help the operator with needle insertion to achieve a homogeneous distribution of up to five fibers in the nodule. The procedure is generally performed with local anaesthesia (2-5 mg of 2% lidocaine) and/or under conscious sedation, even though some authors prefer not to use any kind of anaesthesia, in order to better monitor the procedure during ablation [39]. Once the procedure has been planned, one or more 21-G introducer needles are placed in the deeper portion of the target nodule under real-time ultrasound guidance. If multiple insertions are performed, a distance of approximately 1 cm is maintained between the fibers [40,41]. Then, a plane-cut quartz optical fiber is inserted and advanced up to the introducer needle tip. The introducer needle is then partially retracted to expose the fiber tip by at least 5 mm. A safety distance of about 10-15 mm should be left between the fiber tip and any critical structures to avoid potential complications. The first illumination is generally directed into the deepest part of the nodule, with a fixed power protocol of 3 W, and a total energy delivered for each fiber/illumination between 1,200 and 1,800 J. During treatment, gas formation is continuously monitored in real time with ultrasound. Laser fibers are subsequently retracted one or more times to cover the entire volume of the nodule. This technique is also known as the "pull-back technique," and has the advantage of reducing the number of direct punctures of the nodule, the invasiveness of the procedure, and patients' discomfort.
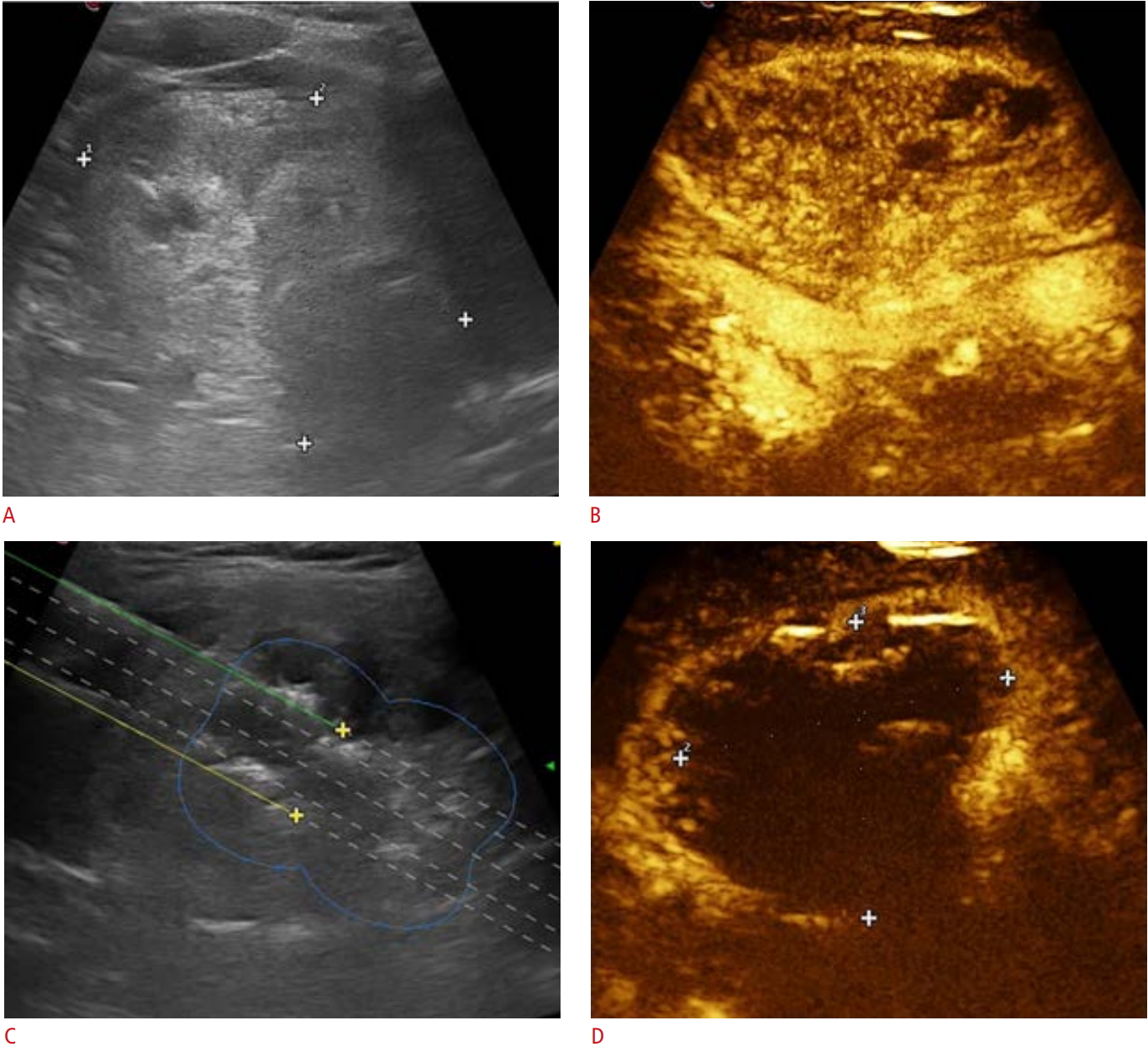
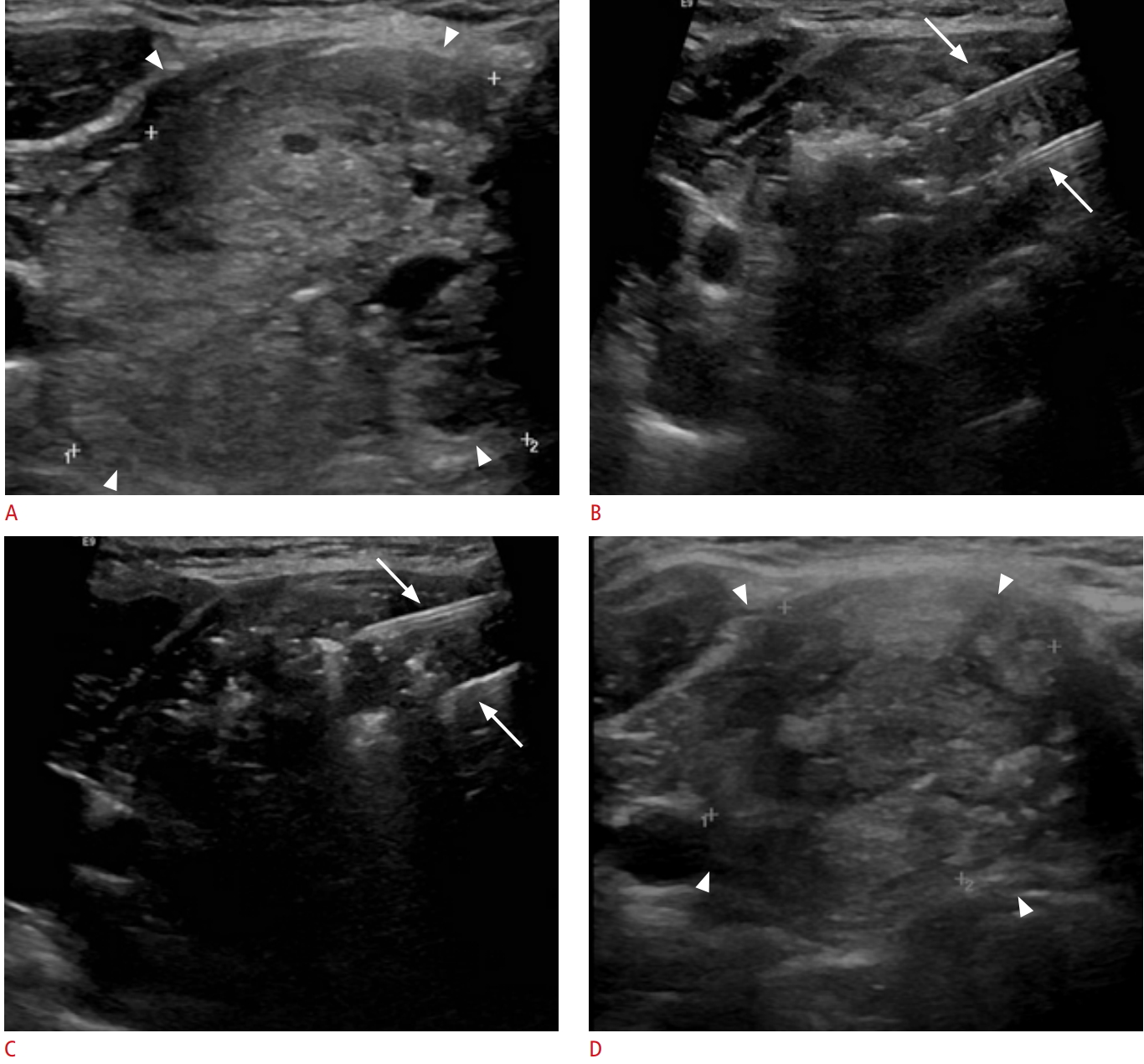
After ablation is completed, contrast-enhanced ultrasonography (CEUS) can be performed in order to precisely assess the ablated volume, and in case of residual vital tissue, ablation can be completed under CEUS guidance [42-44]. Patients are generally kept under observation for a couple of hours after the procedure and then discharged from the hospital. Two cases of benign thyroid nodule treatment with LA are shown in Figs. 1 and 2.
Unlike benign nodules, the purpose of treating malignant nodules is to ablate the whole nodule volume, including safe margins of at least 3-5 mm. This implies the need for additional care in the identification and preservation of the surrounding vital structures. Ideally, malignant nodules should be at least 5 mm distant from the thyroid capsule for LA to be suitable. Ablation is then performed with the same protocol described above to treat benign nodules [16]. However, in this setting, the use of CEUS is of paramount importance, as it allows the detection of areas of the nodule that still need to be treated [45,46].
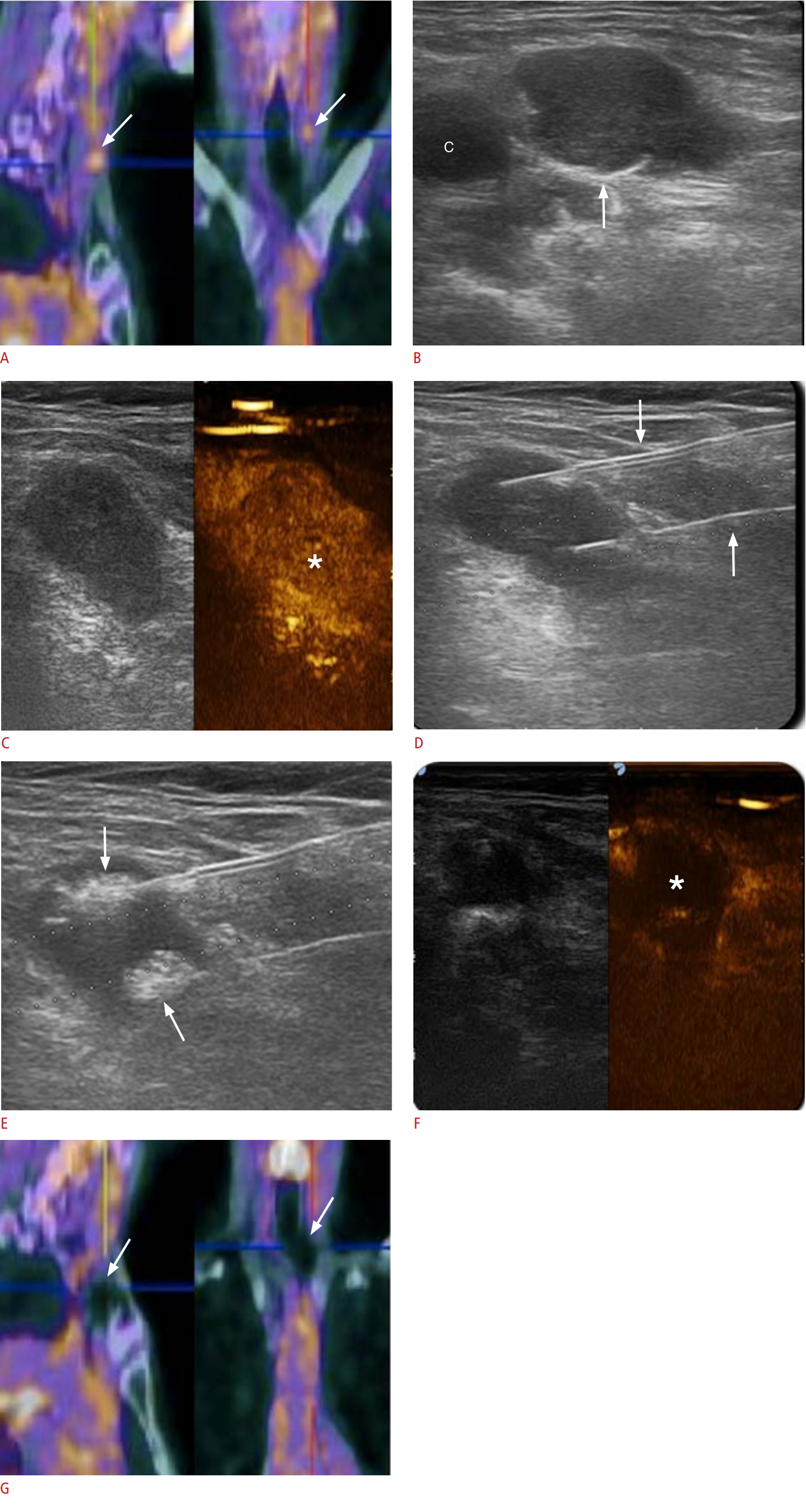
In cases of recurrent thyroid tumours or lymph node metastases, target lesions can be adjacent to critical structures. In such cases, a variable amount of fluid solution ("hydrodissection") can be injected between the lesion and the structure to preserve to increase their distance [47-49]. Then, ablation can be performed with a 3 W fixed protocol and 1,200-1,800 J, with one or multiple fibers. Ultrasound monitoring and CEUS are crucial for the safety and success of this procedure, while fusion imaging might help increase visibility for deeper lesions [24,46,50,51]. A case of a recurrent thyroid cancer treated with LA is shown in Fig. 3.
Results of LA in the Thyroid
Benign Nodules
Several papers on initial experiences demonstrated the efficacy of LA for inducing volume shrinkage of benign thyroid nodules over time. In 2007, a prospective randomized controlled trial by Papini et al. [52] analyzed 1-year changes in nodule volume and the modification of local symptoms in patients with benign solid thyroid nodules randomly assigned to LA, levothyroxine therapy, or observation. The authors found significant nodule volume reduction (change in volume, -5.2±3.1 mL vs. -0.6±2.2 mL vs. 0.7±2.2 mL, respectively), with good treatment toleration by patients and better improvement of local symptoms in the LA group than in controls (81% vs. 13.3% vs. 0%) [52]. A retrospective study by Achille et al. [43] reported a mean nodule volume reduction from 24.2±19.4 mL to 6.2±6.6 mL at 6 months (P<0.001) and to 4.5±5.2 mL at 12 months (P<0.001), with an overall mean nodule volume reduction at the end of the study of 84%±13%. Complete resolution of cosmetic concerns was found in 87% of participants, and pressure symptoms were resolved in 88% [43].
The volume reduction achieved with LA has been shown to be stable over time, with protracted clinical benefits even after a single treatment. A prospective multicentre randomized trial investigating the long-term results of LA of benign thyroid nodules reported volume reduction in comparison with the baseline volume of 49%±22%, 59%±22%, 60%±24%, and 57%±25% at 6, 12, 24, and 36 months, respectively (P<0.001). The 36-month follow-up documented a ≥50% reduction in 67.3% of the treated nodules (P<0.001). At that time, local pressure symptoms were present in 8% of patients, compared to 38% at baseline [30]. Approximately 5% of the nodules treated with LA presented partial regrowth over time. A retrospective study by Dossing et al. [53] analyzed 78 patients with a benign solitary solid nodule treated by LA and observed them for a mean follow-up of 36 months (range, 12 to 96 months). The overall median nodule volume decreased from 8.2 mL (range, 2.0 to 25.9 mL) to 3.5 mL (range, 0.6 to 17.6 mL) after 12 months (P<0.001) and to 4.1 mL (range, 0.6 to 33.0 mL; P=0.001) at the final evaluation. At that time, the median reduction was 51% (range, -194% to 95%). Almost all patients included in the study had pressure symptoms, which disappeared in 84% of cases. Cosmetic concerns disappeared in 72% of patients. Both the self-reported pressure symptoms (r=0.4, P=0.02) and the cosmetic complaints (r=0.3, P=0.02) were significantly correlated with nodule volume reduction after LA [53]. In a prospective, single-centre study, Oddo et al. [54] investigated changes in quality of life after LA treatment of benign thyroid nodules. The authors reported a significant improvement of visual analogue scale scores in all patients after 1 week, and a significant improvement in goitre symptoms and in the general score after 1 and 6 months, as evaluated by the Thyroid-specific Patient Reported Outcome questionnaire.
One of the main issues of IGTA in benign thyroid nodules is the possible regrowth of the treated nodule over time [20]. With LA as well, regrowth of the marginal unablated nodule tissue may occur, and particularly in case of initially large nodules, subsequent treatment can be necessary [55]. As a general rule, retreatment is indicated in cases of incomplete symptom relief, volumetric reduction <50%, and nodule re-growth [20]. Compared with other ablation techniques, such as RFA, LA seems to provide similar results, with a possible trend for a lower complication rate and less discomfort. In 2015, a systematic review including traditional pooling and a Bayesian network meta-analysis of the comparative efficacy of RFA and LA was published, reporting apparent superiority of RFA in reducing benign thyroid nodule volume [56]. However, that paper was based on old results on LA (up to 2007), and mainly on the experiences of a single centre (5 out of 7 papers in the LA group were from the same centre). Subsequently, in a single-centre study comparing 90 patients treated with percutaneous LA or RFA by the same group of operators, no difference in the time course of the relative volume reduction between the two techniques was found [40]. A recent multicentre study, aimed at comparing the effect of LA and RFA through a propensity score matching analysis, evaluated data from 601 consecutive patients (449 LA and 152 RFA). In that study, the mean nodule volume decreased from 21.5±16.5 mL at baseline to 8.7±7.7 mL (P<0.001) and to 8.0±7.2 mL (P<0.001) at 6 and 12 months, respectively, in patients who underwent LA, and from 24.5±17.9 mL at baseline to 11.3±10.7 mL (P<0.001) and to 9.9±9.5 mL (P<0.001) at 6 and 12 months, respectively, in patients who underwent RFA. No significant differences in volume reduction at different time points was found between the two groups [57]. Therefore, based on the more recent literature, the two techniques can be considered equivalent in terms of results for nodule volume reduction when performed by experienced operators.
The safety of LA has been investigated in several studies, which have found high levels of tolerability and low numbers of major complications. A multicentre retrospective analysis of 1,837 treatments from eight centres found an overall complication rate of 0.9%, with no life-threatening complications [55]. Major complications occurred in 0.5% of cases (8 patients), and all consisted of voice changes due to vocal cord palsy, with complete recovery after 3 months. Minor complications were reported in 0.5% of cases (9 patients), including subcapsular or perithyroidal hematoma and skin burn. Pain was the most frequent side effect of LA and was recorded as mild or moderate, respectively, in 10.6% and 1.6% of patients.
LA can also be successfully used to treat patients with benign hyperfunctioning thyroid nodules. In a recent paper, Gambelunghe et al. [28] reported 3-year results after LA of 82 patients with hyperfunctioning thyroid nodules. They found significant volume reduction of the treated nodules from 12 mL (range, 5 to 118 mL) to 5 mL (range, 1.2 to 40 mL) after 3 years (P<0.001). Notably, better results were achieved in smaller (<15 mL) nodules, where the percentage of ablated tissue was higher. Thus, with proper patient selection, LA also seems to be a valuable alternative for the treatment of hyperfunctioning thyroid nodules [58]. Furthermore, a recent pilot study comparing outcomes in patients with large toxic nodules treated with LA followed by 131I with those treated by 131I alone showed that combined treatment might induce a faster resolution of systemic and local symptoms than 131I alone. In addition, for three patients, no 131I treatment was needed after LA [27].
Malignant Thyroid Tumours
Even though surgical excision remains the first therapeutic option in patients with thyroid cancer, both for primary disease and for recurrence, in recent years LA has been successfully applied to treat patients unsuitable for surgery with promising results [17,24,28]. The incidence of thyroid cancer has increased in the last decades, but without a concomitant increase in mortality. This fact might well reflect an increase in the early diagnosis of indolent tumours, which might have never affected the patient's life. Thus, these tumours, which once detected generally require surgical treatment, can be regarded as overdiagnosed and overtreated [16,59-62]. In order to reduce the adverse events associated with overtreatment, some authors have suggested applying an active surveillance strategy to small micropapillary thyroid carcinomas [63-65]. In between these two strategies, percutaneous thermal ablation has been proposed as a possible strategy of care, minimising the invasiveness of the treatment, in order to compensate for overdiagnosis and to reduce the negative effects of overtreatment [66,67].
Lee et al. [68], in an ex vivo study, performed LA immediately after thyroidectomy in three patients with papillary thyroid cancer. Histological analysis of the specimens demonstrated no viable tumour cells, and tumour safety margins comparable to those obtained through surgery. In 2011, Papini et al. [16] treated an incidental papillary thyroid microcarcinoma (PTMC) with LA in a patient at high surgical risk. The procedure was well tolerated, without complications. Ultrasound-guided fine-needle aspiration biopsy and core-needle biopsy performed 12 months after LA demonstrated necrotic material and inflammatory cells with no viable neoplastic cells [58]. Valcavi et al. [17] treated 3 patients with a single PTMC in the operating room under general anaesthesia immediately before surgical removal of the thyroid gland. In all cases, pathology demonstrated irreversible damage of the ablated neoplastic tissue. However, in two cases, papillary microfoci were identified in the removed thyroid gland, and in one case a lymph node micrometastasis was observed. This highlights one of the main issues of IGTA in thyroid malignant tumours, which is related to the inability of ultrasonography to detect very small tumour foci within the thyroid or in locoregional lymph nodes. Subsequently, Zhang et al. [45] published a larger series of 64 cases of PTMC treated with LA. Two incomplete ablations were detected by CEUS performed immediately after the procedure and a complementary ablation was successfully performed. Ultrasound-guided fine-needle aspiration at 1, 6, and 12 months after treatment did not show any residual tumour. No regrowth of treated lesions could be detected during a mean follow-up of 25.7±8.2 months (range, 12 to 42 months).
A cervical metastatic lymph node was detected on ultrasound and cytologically confirmed at 30 months after treatment [45]. Thus, even if the present evidence is limited, LA seems to represent a feasible and valuable therapeutic option for the treatment of small PTMC. LA has also been demonstrated to be safe and effective for treating recurrent papillary thyroid carcinomas (PTCs) [69] (see Table 1). Zhou et al. [70] published a retrospective study, conducted in 21 patients with 27 recurrent PTC lesions treated with LA. Recurrent PTCs were identified during routine ultrasound follow-up after surgery. Twenty-four lesions received one ablation each and were completely ablated. Three incompletely ablated lesions detected on CEUS received a subsequent successful ablation. The mean follow-up was 14.9±5.9 months (range, 6 to 24 months) [70]. In metachronous cervical nodal metastases from PTC, LA may reduce or delay highly invasive repeat neck dissections, especially in high-risk patients. In 2013, Papini et al. [15] reported on the treatment with LA of five patients with previous total thyroidectomy and neck dissection, with eight new lymph node metastases with a volume less than 5 mL and no radioiodine uptake at a post-therapeutic 131I whole-body scan. A single LA was carried out without major complications. Treatment induced the progressive shrinkage of metastatic lymph nodes in all patients and no regrowth of the successfully treated lesions was detected. Colour Doppler and CEUS studies demonstrated an absence of vascularization. Mauri et al. [24] used LA to treat 24 patients with elevated serum levels of thyroglobulin or anti-thyroglobulin antibodies and a total of 46 metachronous nodal metastases. All patients had previously undergone surgery and radioiodine ablation, were at high surgical risk, and had a negative radioiodine scan. The authors obtained technical success in all 46 lymph nodes (100%) with no major complications. Thyroglobulin levels decreased from 8.40±9.25 ng/mL before treatment to 2.73±4.0 ng/mL after treatment (P=0.011), with serological conversion in 11 of 24 patients (45.8%). Local control was obtained in 40 of the 46 lymph nodes (86.9%) over a follow-up of 30±11 months, and no residual disease was identified on imaging in 19 of 24 patients (79.1%). Local control was achieved in 40 of the 46 lymph nodes (86.9%) at 1 year and in all of the 25 nodes (100%) that were followed for 3 years, with an estimated mean time to progression of 38.6±2.7 months.
Conclusion
In conclusion, LA is a feasible, safe, and effective technique for the treatment of benign thyroid disease. LA may lead to resolution of clinical symptoms in the vast majority of cases, with reduced invasiveness, a low complication rate, and maintenance of gland function. Thus, this treatment can be considered as an effective alternative to surgery in patients with benign thyroid nodules. Additionally, it may be possible to use LA safely in the treatment of malignant thyroid cancer, both primary and metastatic. However, the evidence of efficacy of LA in malignant disease is still limited, and at present, this technique can only be considered after careful multidisciplinary evaluation in cases not suitable for standard therapies.
 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



