

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
The glenohumeral joint (GHJ) is a frequent site of pain and pathology with a reported prevalence from 7% to 23% in adults [1,2]. GHJ osteoarthritis can affect up to 33% of people over 60 years of age [3,4] and adhesive capsulitis affects 2%-5% of the general population and 10%-15% of individuals with diabetes [5,6]. In adhesive capsulitis, the capsule becomes contracted and thicker, particularly in the infraglenoid recess and rotator cuff interval [7-9], which limits joint mobility [10]. Inferior capsule thickening of more than 3.5 mm recorded using ultrasound is 66.7% sensitive and 92.5% specific for the diagnosis of shoulder adhesive capsulitis [11]. Capsular tissue elasticity affects range of motion (ROM), or the allowed amount of joint plane-specific motion (e.g., GHJ flexion), more than thickness, indicating a need for capsular tissue stiffness measurements [12]. Capsular tightness restricts joint ROM and increases joint contact pressures, leading to intra-articular pathology [13] and limiting the ability to complete basic activities, such as dressing and hygiene [3]. Clinicians commonly manage patients with ROM limitations, functional impairments, and pain using stretching and joint mobilization techniques [14-16]. Several authors [17-19] reported that GHJ mobilization using loads of 20-80 N increased capsule extensibility or elongation and improved patient symptoms [20,21]. The proposed mechanical and neurophysiological changes responsible for increased joint ROM following joint mobilizations are not well understood and require further investigation [22]. Shear wave elastography (SWE) measurements are a reproducible method of evaluating muscle and tendon [23-26], with good repeatability, as demonstrated by intraclass coefficients (ICCs) of 0.81-0.91. This allows SWE to provide information on tissue diagnosis, injury, and/or healing states [27,28]. However, no study has validated SWE readings in capsular tissue against a reference standard. Therefore, the purpose of this study was to investigate: (1) the reliability of SWE measurements of GHJ capsular tissue under various loads; and (2) the degree of correlation between measurements of GHJ capsular tissue tension properties under various loads made using a durometer versus SWE.
Materials and Methods
This study was approved by the Ethics Sub-committee of the Department of Anatomy at the Université du Québec à Trois-Rivières, Trois-Rivières, Québec and exempted by the University of North Texas Regional Institutional Review Board. A convenience sample of 10 frozen GHJ specimens (5 right and 5 left) was acquired from five fresh cadavers through the Department of Anatomy at the Université du Québec à Trois-Rivières. The specimens included four males and one female, with a mean age of 77.8±5.4 years, height of 1.65±0.09 m, weight of 59.6±15.67 kg, and body mass index of 21.6±5.31 kg/m2.
The inferior capsular attachment to the humerus and scapula was excised along with the GHJ capsule to allow for testing. The samples were then trimmed to a 12-mm width for testing. The specimens were then placed in containers and frozen in storage until needed at -20℃. Tissue specimens were thawed for 1-2 hours and then tested at room temperature (18℃). Tissue specimens were connected to a standing frame using a custom clamp and a rope with the attached load (Fig. 1) along with a random selection of 1-, 3-, 5-, and 8-kg loads for measurements using SWE and the durometer. Investigators recording the durometer and SWE measurements were blinded to the loads applied to the tissue samples.
SWE Measurements
The SWE procedures were performed at a regional health and social services center (Centre Intégré Universitaire de Santé et de Services Sociaux de la Mauricie-et-du-Centre-du-Québec). An Aixplorer (SuperSonic Imagine, Aix-en-Provence, France) diagnostic device was used, with an XL-15-4 linear transducer that allowed the investigator to quantify tissue elasticity without probe compression. The investigator performing the SWE measurements was a medical physicist with over 8 years of experience using SWE and 10 years of image processing.
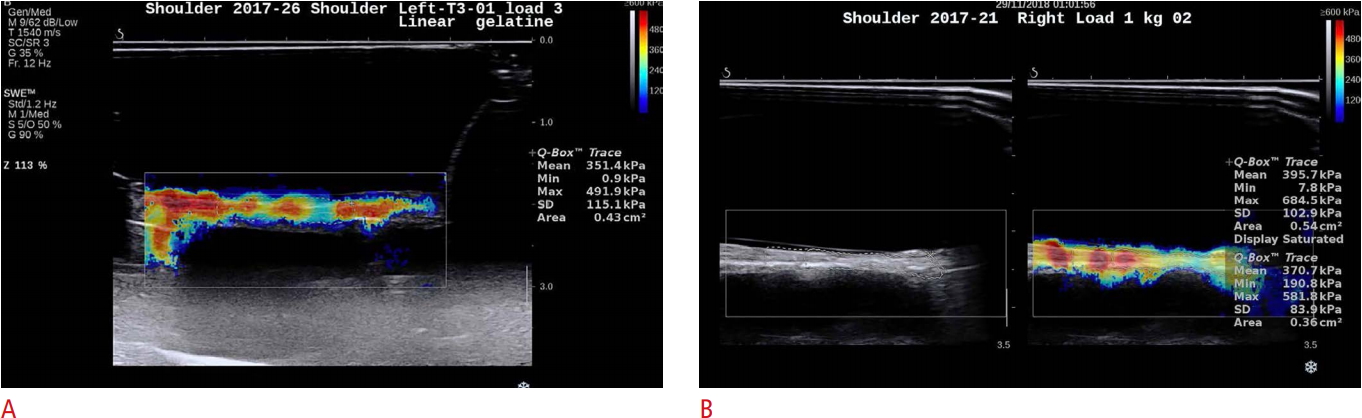
Ultrasound gel was placed on the sample tissue followed by application of a conforming gelatin pad, and the specimen was secured with Opsite Flexifix (Smith & Nephew, Andover, MA, USA) (Fig. 2). The ultrasound gel was applied to the Opsite covering and then visualized with B-mode ultrasound. Once an acceptable image of the capsular tissue was achieved, the SWE was activated and the image scanned for best resolution. Once the region of interest (ROI) was identified in the Q-box, which provides the field of view, the probe was removed. The ROI was then marked and saved using the Q-box tracer and used to acquire a measurement of elasticity (kPa) within the Q-box data area. Data were obtained for five measurements from each tissue specimen using loads of 1, 3, 5, and 8 kg for the shoulder in three trials to assess reliability (Fig. 3). The reliability and correlation analyses were calculated using the mean measurements obtained for each load of each trial.
Durometer
The Shore A durometer (HT-6510A Shore A, Tongbao, Shenzhen, China), a digital, hand-held, spring-loaded device (Fig. 4), was calibrated, and the pressor was applied parallel to mid-portion of tissue specimens and held in contact for 1-2 seconds until a measurement was obtained. This was repeated for five measurements using randomly selected 1-, 3-, 5-, and 8-kg loads in two trials separated by at least 5-minute intervals by a blinded investigator to assess reliability. Data were recorded for five measurements from the tissue specimens at each load in three trials to assess reliability (Fig. 4).
Descriptive statistics including mean, median, standard deviation, ranges, and minimum/maximum values were calculated for the durometer and SWE measurements. The reliability of the durometer and SWE measurements was established using the intraclass correlation coefficient (ICC3,5). Data normality was assessed using the Shapiro-Wilk test, which indicated that the SWE and durometer measurements were normally distributed for the 1-, 3-, and 5-kg loads (SWE, P=0.572-0.960; durometer, P=0.441-0.730), and the kurtosis and skewness coefficients were lower than ±1. Therefore, the associations between SWE and durometer measurements were assessed with Pearson correlation coefficients. Statistical significance was set at P<0.05 for all analyses. All data and statistical analyses were performed using IBM SPSS statistics version 23 software (IBM Corp., Armonk, NY, USA).
Results
The SWE and durometer measurement values are shown in Table 1.
The intra-day reliability of the durometer measurements was 0.90 (95% confidence interval [CI], 0.79 to 0.96; P<0.001) and that of the SWE measurements was 0.95 (95% CI, 0.88 to 0.98; P<0.001). A moderate correlation was observed between the durometer and SWE tissue tensile loading measurements at 1 kg (r=0.56, P=0.095), 1 and 3 kg combined (r=0.72, P<0.001), and 1, 3, and 5 kg combined (r=0.62, P<0.001), with a slight correlation at 3 kg (r=0.36, P=0.313). The 5-kg load demonstrated a moderate negative correlation (r=-0.56, P=0.089), which can likely be explained at least partially by the 800-kPa maximum SWE limit causing a ceiling effect. The 8-kg load could not be measured consistently due to tissue thinness with loading and SWE sample saturation with the 800-kPa measurement limit.
Discussion
This is the first study to assess the reliability of SWE and correlations between the durometer and SWE for GHJ capsular tissue properties under clinically applicable tensile loads using cadaveric tissue to eliminate neuromuscular influences. Tensile loads were selected based on pilot testing of the durometer for capsular tissue with good reliability (ICC3,5, 0.87; 95% CI, 0.68 to 0.95) and a high correlation between the tensile load applied and durometer measurements for loads of 1, 2, and 5 kg, as well as other prior studies of GHJ tissue properties [17,18,29]. The SWE measurements for reliability and correlation in this study were performed by one observer in 1 day. The mean of five successive measurements was used to determine reliability. This design provided the best conditions to determine SWE reliability values. In this SWE study, the machine's Q-box provided measurement selection through identification of the shear ROI. However, when the 5- and 8-kg loads were applied, saturation in some specimens due to the 800-kPa maximum SWE limit affected the mean tissue shear measurements, thereby creating a ceiling effect, which could have affected measurement validity at higher loads. Our findings showed that GHJ capsular tissue measurements under tensile loading using SWE had excellent reliability (ICC, 0.95). These findings suggest that SWE is reliable for measuring GHJ capsular tissue in cadavers during tensile loading. These results are in line with a previous in vivo study that evaluated GHJ capsular thickness and elasticity in two different positions, with an intra-rater reliability value of 0.93 for posterior-inferior capsule elasticity [12].
Previous studies reported ROM changes after mobilization [5,18] and tissue elongation after simulated oscillations [29], but a better understanding of how these interventions affect tissue properties is needed. This study demonstrated that SWE technology may allow non-invasive measurement of tissue changes during joint loading and capsule stretching procedures. Future studies evaluating the effects of tensile loading on capsular tissue in vivo are warranted to determine capsule behaviors during various mobilizations and whether changes in tissue properties are maintained post-loading.
A durometer measures a material’s hardness or resistance to deformation by applying an indentation load on the specimen, giving a measure of tissue hardness based on an arbitrary Shore unit (HA) [30,31]. Durometers have been used in various medical applications, such as in dermatology [32,33] and for measurements of organ [34-36], breast [37], and muscle [38] tissue. The intra-rater and inter-rater reliability measures of durometer measurements of epidermal tissue were good to excellent [32,33]. However, reliability has not been established in capsular tissue. Likewise, GHJ capsule hardness measurements with a durometer had high intra-rater reliability (ICC, 0.90) and could be used as a control method to validate diagnostic methods such as SWE [34]. These findings establish the durometer as a reliable and simple tool for measuring capsular tissue hardness in vitro. Selected durometer measurements at higher loads were difficult to obtain due to tissue sample thinness, which affected the consistency of the measurement location in some specimens. This may explain why the reliability coefficients were not as high as those reported by Kissin et al. [33]; however, our results were at the higher part of the range reported by Merkel et al. [32] for epithelial tissue measurements.
A modest correlation was observed between SWE and durometer measurements of GHJ capsular tissue stiffness and hardness for the 1-kg load and the 1- and 3-kg loads combined, and a small correlation was found with the 3-kg tensile loads. This indicates that as the load increased, GHJ capsule stiffness as measured by SWE and hardness as measured by the durometer increased at lower loads. Similar correlation values between B-mode ultrasonography and durometer measurements were reported in muscle tissue [38], indicating that both modalities measure different parameters that are closely related to the modulus of elasticity. Achilles tendon tensile loads and SWE have been moderately correlated under progressive loads [39]. In the current study, the 5-kg tensile load resulted in a moderate negative correlation between the durometer and SWE measurements; these results should be viewed with caution due to tissue thinness, inconsistencies in the location of the durometer and SWE measurement locations, and SWE saturation levels at the 5-kg tensile load.
There are some advantages of using SWE to evaluate joint capsule properties. First, it is a reliable measurement modality and can conveniently and quickly assess the elastic properties of a joint capsule. In the present study, the time required for scanning and evaluating the capsule was only a few minutes. These advantages make SWE a promising modality to diagnose capsular pathology and to evaluate treatment progression and the efficacy of different interventions.
There were some limitations to our study. Soft tissues around the capsule were removed by hand and although great care was taken to clear other tissue from around the capsule, any remaining noncapsular tissue could have contributed to some load resistance. Studies evaluating whether such properties are maintained over time and using other joint capsular tissue would be valuable. Further research is needed to determine the effects of tensile loading on capsular tissue and to provide insight into the effects of stretching and joint mobilization loads on joint ROM changes in vivo.
In conclusion, SWE is a simple and reliable method of measuring the elastic properties of the GHJ capsule in cadaveric tissue. Additional research is required for the evaluation of capsular tissue tension properties during and following various loads, without the interference of the neuromuscular system, using SWE.



 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



