

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
The round ligament of the femur, also known as the ligamentum teres femoris, is a pyramidal or quadrangular intra-articular ligament of the hip. It originates from the acetabular notch and the transverse acetabular ligament and inserts into the fovea capitis of the femur [1-4]. In recent decades, the development of hip arthroscopy has led to increased interest in the role of the round ligament in hip pain and stability. Tearing of this ligament is a major source of hip pain [5-8], constituting the third most common cause of hip pain in athletes who have undergone diagnostic arthroscopy [7,9]. Free nerve endings in the round ligament have been suggested to mediate components of the pain response in degenerative arthritis. It is also well established that lesions of the round ligament can cause hip pain in the absence of any other hip pathology. The treatment methods for such lesions are still evolving. Currently, surgical intervention is effective in the majority of patients with round ligament lesions, and the most common procedure is arthroscopic debridement using radiofrequency ablation [7,10].
Ultrasonography-guided intra-articular steroid injection in the hip (UISIH) is a conservative option for the management of hip pain. The effect of UISIH in patients whose sole cause of hip pain is round ligament injury, however, has not been reported. Only a few articles have investigated the effect of steroid injections in the hip for the treatment of osteoarthritis [11]. To the best of our knowledge, the present study is the first to demonstrate the effectiveness of UISIH in patients with a partial tear or degeneration of the round ligament.
Materials and Methods
All subjects with hip pain underwent a standard evaluation that included a clinical examination as described by Martin and Palmer [12]. If a further examination was needed, imaging studies such as X-ray imaging, computed tomography, or magnetic resonance imaging (MRI) were recommended. Patients whose conditions warranted conservative treatment received medication and physiotherapy. However, when the symptoms failed to improve or the physician deemed it necessary, UISIH was performed [13]. We obtained approval for the retrospective review of patients’ records from the local institutional review board, and the requirement for patients to provide informed consent was waived.
Patient Population
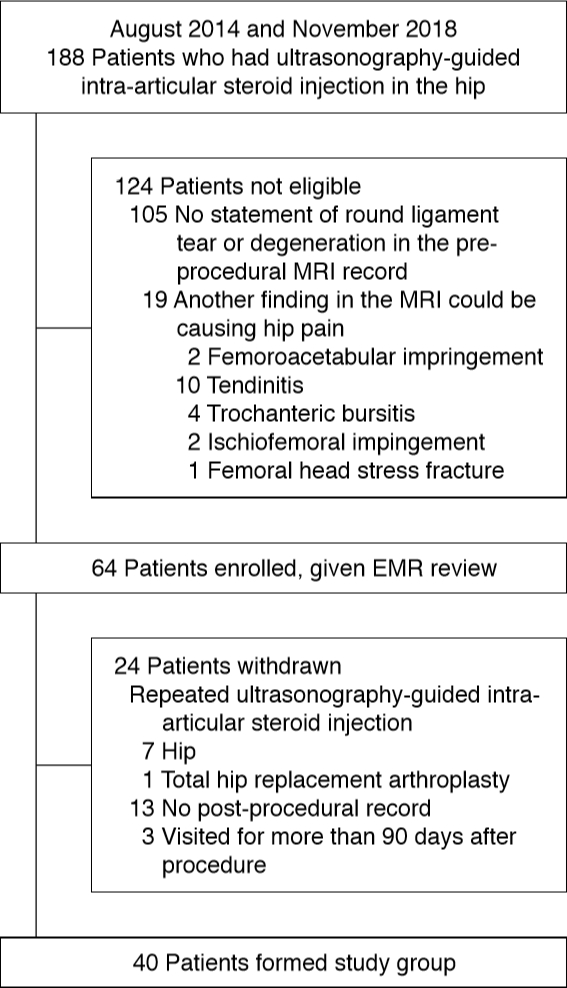
We identified a total of 188 patients who underwent UISIH between August 2014 and November 2018. First, we excluded 105 patients who showed no evidence of partial round ligament tear or degeneration on pre-procedural MRI, including two cases of complete round ligament tear. Next, we excluded 19 patients who displayed additional MRI findings that could be responsible for hip pain, namely femoroacetabular impingement, calcific tendinitis, trochanteric bursitis, ischiofemoral impingement, or femoral head stress fracture. Then, seven patients who had been treated with repeated UISIH and one patient who had undergone total hip replacement arthroplasty were excluded. Thirteen patients who had no post-procedural records and three patients who were followed up for longer than 90 days after the procedure were also excluded. Ultimately, 40 patients who met all criteria were included in this study (Fig. 1). The study population comprised 19 men and 21 women (52.5%), with a mean age of 48 years (range, 20 to 76 years) and an average follow-up duration of 43 days (range, 15 to 90 days). Thirteen patients underwent steroid injection into the left hip joint and 27 into the right.
Image Analysis
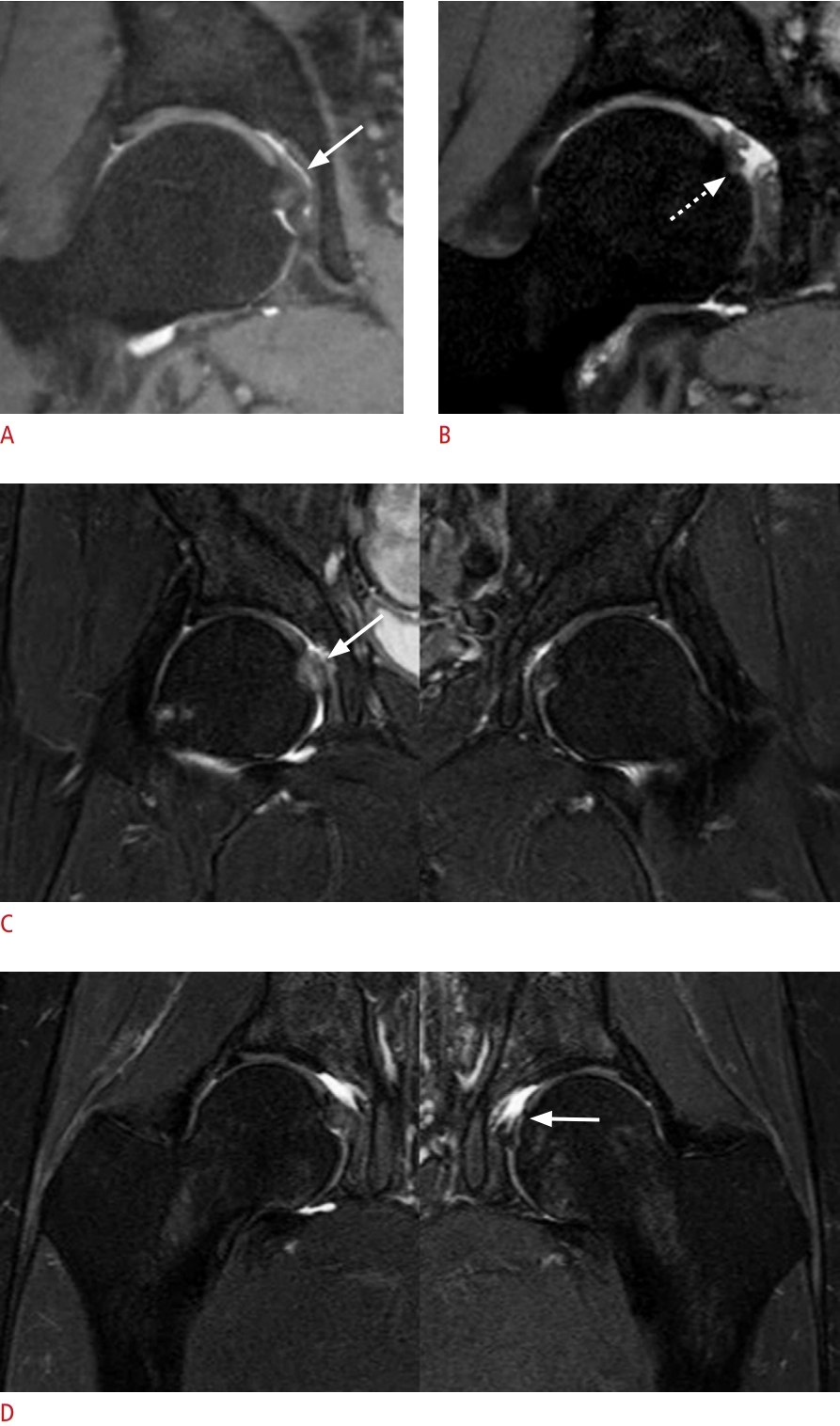
We retrospectively reviewed pre-procedural MRI records analyzed by six musculoskeletal radiologists with 2 to 17 years of experience to determine if patients displayed round ligament tears or degeneration. Two musculoskeletal radiologists then came to a consensus regarding the presence of round ligament tearing or degeneration as follows. Partial tears, degeneration, and complete tears were characterized by different MRI findings. A partial tear was defined by torn fibers or marginal irregularity accompanied by focal insufficient thickness of the ligament compared to the contralateral side [2]. Degeneration was defined by a marked increase in signal intensity on proton density-weighted fat-suppressed imaging and T2-weighted fat-suppressed imaging or swelling relative to the contralateral side [2]. A complete tear was defined by the complete absence of ligamentous material or a full-thickness disruption of the normal pathway between the fovea capitis and the transverse ligament [2,14]. Normal round ligaments were defined by the presence of intact fibers with normal origin and insertion, normal thickness, homogeneous hypointense signal intensity with all pulse sequences, and smooth margins. Fig. 2 shows an example MRI image from one patient each with round ligament degeneration, a partial tear, a complete tear, and normal findings. In addition, we reviewed causes of hip pain other than round ligament tear or degeneration on MRI to exclude the compounding factors of femoroacetabular impingement, calcific tendinitis, trochanteric bursitis, ischiofemoral impingement, and femoral head stress fracture [15].
Injection Technique
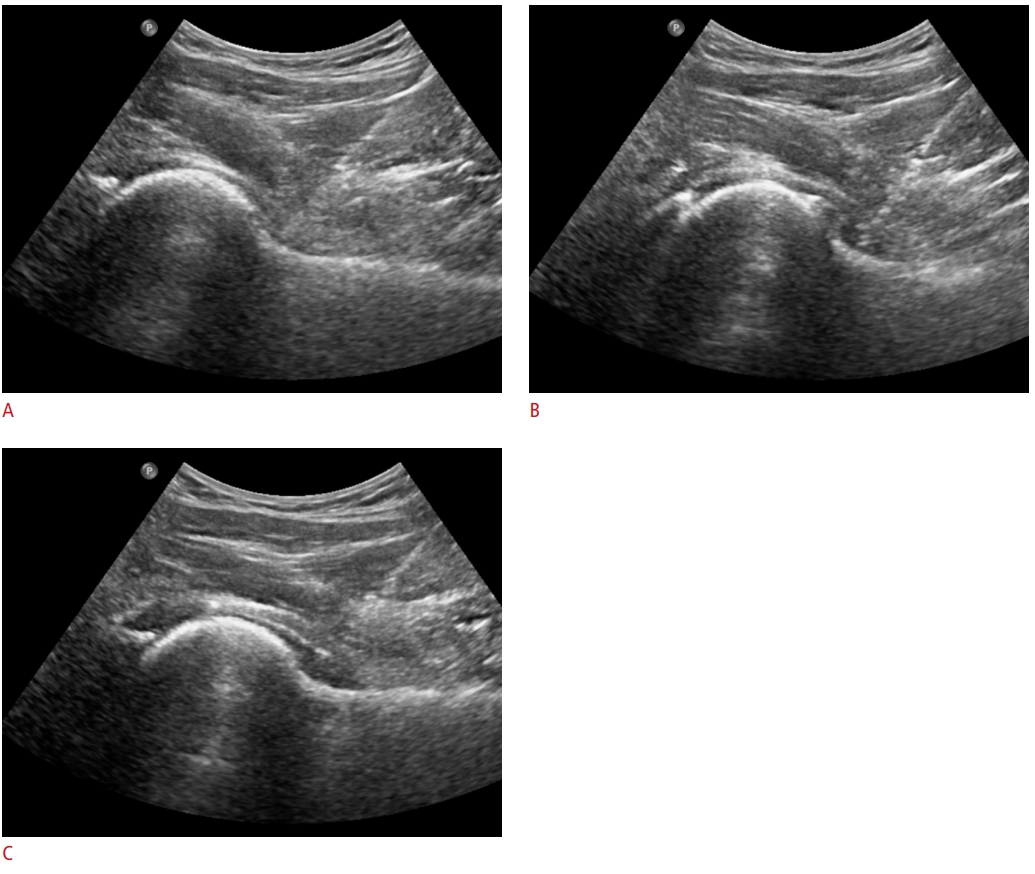
Each patient lay on a bed in the supine position with the hip slightly abducted and the knee pointed forward. All UISIHs were conducted by an experienced musculoskeletal radiologist (Y.C.Y.) using an iU22 ultrasound scanner (Philips, Bothell, WA, USA) equipped with a C5-1 MHz curved array transducer. A survey scan was first performed to determine the entry point of the needle. First, to identify the femoral head, the transducer was placed on the inguinal area parallel to the inguinal ligament. Then, the probe was rotated internally with the probe marker aimed toward the umbilicus until the femoral head, neck, and anterior capsular recess aligned in a single plane. The groin area was sterilized with a cotton ball soaked with 2% chlorhexidine-alcohol and covered with a sterile cotton surgical drape centered on the planned needle entry point. The transducer was covered with a sterile ultrasound probe cover. With the probe held in an oblique longitudinal orientation so that the femoral head and neck aligned in a single plane, 2-3 mL of local anesthetic (lidocaine hydrochloride, 200 mg/20 mL; Daihan Pharmaceutical Co., Ltd., Seoul, Korea) was injected at the planned needle entry point to minimize the pain of spinal needle insertion. Next, the spinal needle (Quincke Bevel, 22-gauge 3-1/2 inch; TaeChang Industrial Co., Ltd., Gongju, Korea) was inserted using an in-plane approach to target the anterior capsular recess under real-time ultrasound guidance. When the needle tip was positioned inside the joint capsule, 1 mL of saline loaded in a 5-mL syringe was injected to confirm successful targeting of the joint space. Following this, 1 mL of triamcinolone acetonide (Tamceton, 40 mg/1 mL; HanAll Biopharma Co., Ltd., Seoul, Korea), 2 cc of 1% lidocaine, and 5 mL of normal saline (sodium chloride, 180 mg/20 mL; Huons Co., Ltd., Seongnam, Korea) were flushed through the extension tube. To reduce the possibility of chondrotoxicity by local anesthetics, which can be impacted by exposure time and concentration, we chose short-acting 1% lidocaine and diluted it with 5 mL of normal saline. The injection was considered a technical success when the hyperechoic material generated by the steroid particles was observed below the joint capsule on real-time ultrasound imaging conducted after the procedure. We also checked for the presence of immediate complications such as hematoma on the post-procedural scan (Fig. 3).
Review of Clinical Data
Short-term relief from symptoms was retrospectively evaluated at the first follow-up appointment after UISIH. One author reviewed patients’ electronic medical records to assess their subjective experience of symptoms, which were classified on a 5-point scale as follows: 0 (aggravated), 1 (unchanged), 2 (symptoms improved but cannot be ignored), 3 (greatly improved; negligible symptoms), and 4 (no residual symptoms). The use of a 5-point scale was based on an article by Lee et al. [16], and the scale was constructed in reference to the Mankoski Pain Scale (2000) [17]. A score of 0 (aggravated) was assigned if the patient described experiencing any aggravation of pain. A score of 1 (unchanged) was defined as including mentions of the pain being the same as before the procedure or unchanged from before the procedure. A score of 4 (no residual symptoms) was assigned based on mentions of a lack of problems with hip joint pain and motion. Of the patients not already classified as 0, 1, or 4, those who used positive language and whose descriptions of remaining symptoms indicated that they were mild (with word choice such as "little" or "negligible") were assigned a score of 3 (greatly improved; negligible symptoms). The remaining patients were scored as 2 (symptoms improved but cannot be ignored). If descriptions were ambiguous or a local dialect was used, two radiologists assigned a score through consensus. Patients who had a reduction of at least 2 out of 5 points were determined to have experienced symptom reduction. The same author also assessed the incidence of complications after the procedure.
Statistical Analysis
The only continuous variable analyzed in this study was follow-up duration, and it was expressed as mean±standard deviation. Age was categorized into three groups: 20 to 39 years, 40 to 59 years, and 60 years and older. Categorical variables were expressed as frequencies and percentages. The relationship between symptom relief and follow-up duration was analyzed using the t test. The relationships between symptom relief and categorical variables such as age, sex, and injection side were analyzed using the chi-square test and the Fisher exact test. A P-value <0.05 was considered to indicate statistical significance. Statistical analysis was conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Results
The average follow-up periods of all 40 patients and of the patients who experienced symptom relief were 43 days (range, 15 to 90 days) and 44 days (range, 15 to 90 days), respectively. No side effects of the injections were noted. UISIH was administered on the right side in 27 patients (32.5%) and on the left side in 13 (67.5%). The overall technical success rate of the injections by the musculoskeletal radiologist was 100%.
With respect to subjective symptom relief, five patients exhibited unchanged symptoms, 13 experienced improved symptoms, 12 experienced greatly improved symptoms, and five exhibited no residual symptoms. Unsatisfactory results were exhibited by five patients. Thus, a successful outcome was noted in 35 of the 40 patients (87.5%). There were no significant association between symptom relief and sex, age, injection side, or follow-up duration (P>0.05), as shown in Tables 1 and 2.
Discussion
The round ligament, which has long been regarded as a vestigial structure, is a common cause of hip pain and mechanical hip symptoms [18]. The prevalence of round ligament injuries found via hip arthroscopy is 9%. Such damage is classified as complete (type 1), partial (type 2), or degenerative (type 3) [19,20]. Complete round ligament tears typically occur in patients with a history of traumatic or iatrogenic joint disruption. These patients commonly exhibit other intra-articular conditions, such as chondral lesions and labral tears [2,21-23]. Partial round ligament tears are much more common than complete tears and primarily result from mild trauma or repeated stretching. These tears frequently occur as isolated lesions [24]. We excluded patients exhibiting complete tears of the round ligament on MRI.
Pergaminelis et al. [18], Haviv and O’Donnell [25], and Amenabar and O’Donnell [24] have reported that arthroscopic debridement of isolated round ligament tears without resection of the ligament itself potentially reduce inflammation around the torn fibers, thereby relieving pain and improving mechanical function. Intra-articular steroid injections are also used to reduce inflammation. In our study, UISIH is a treatment that is less invasive and much cheaper than arthroscopic debridement and that does not require hospitalization-achieved a successful outcome in 87.5% of patients at the first follow-up visit. No noteworthy side effects of the injections were noted. Therefore, UISIH could potentially be employed for symptom relief before a decision is made about surgery or in patients who are unsuitable for surgical treatment.
Steroids have anti-inflammatory effects, acting on nuclear steroid receptors to interfere with various inflammatory cascades. They reduce vascular permeability; inhibit the accumulation of inflammatory cells, phagocytosis, and neutrophilic superoxide production; and prevent the synthesis and secretion of several inflammatory mediators, including prostaglandins and leukotrienes [26]. Free nerve endings in the round ligament have been suggested to mediate components of the pain response. Thus, steroids may exert direct anti-inflammatory effects on inflamed nerve tissue, inhibiting the accumulation of inflammatory cells and mediators.
A study similar to the present study has been conducted previously. Byrne et al. [27] investigated the effect of intra-articular steroid-bupivacaine injections on knee pain caused by degenerative tears of the medial meniscus and demonstrated reduced pain symptoms in the majority of patients (81.7%).
Our study had a number of limitations. First, it was a consecutive case series study, so it entailed selection bias and included no comparator group. Second, long-term data regarding symptom relief were not analyzed, so the long-term effects of UISIH could not be evaluated. Third, the measured efficacy of the treatment was based solely on subjective symptoms and not on objective measures of functional outcomes. Fourth, we did not evaluate patients’ recovery from mechanical instability following the procedure. Despite its small study population and short follow-up period, we believe that this study is noteworthy, as it is the first to investigate UISIH in patients with a partial tear or degeneration of the round ligament. Given the aforementioned limitations, future prospective studies are required to further evaluate the use of UISIH in the treatment of round ligament injuries.
In conclusion, we demonstrated that UISIH was a safe and effective treatment in patients with a partial tear or degeneration of the round ligament of the femur over the course of short-term follow-up.
 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



