

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Colorectal cancer is the third most frequent cause of cancer-related mortality worldwide [1], and the liver is the most common site of metastasis [2]. Colorectal liver oligometastases (CLOM) is a transitional state of the disease that is generally characterized by the existence of metastases in up to three sites, with sometimes more than five lesions [3]. In these patients, disease control and clinical outcomes can be improved using a local treatment approach, such as ablation. The CLOCC trial (a randomized EORTC [European Organisation for Research and Treatment of Cancer] Intergroup phase II study; EORTC 40004) compared combination treatment (radiofrequency ablation [RFA]+chemotherapy) versus chemotherapy alone [4] and found that the median disease-free survival in the former group was longer (16.8 months vs. 9.9 months, P=0.025). These results lend support to the critical role of ablation in the management of localized disease, which can be considered an efficient treatment to increase survival.
Percutaneous ablation includes a variety of image-guided methods. The most widely used modalities are computed tomography (CT) and ultrasonography (US) for their advantages in speed, facilitation, and visualized observations [5,6]. Each of these two modalities has both advantages and limitations. US guidance is superior insofar as it enables fast, real-time visualization and no radiation. However, there are some "blindspots" or low-visibility areas in the abdomen during ablation, such as the area adjacent to the diaphragm, the gastrointestinal tract, and liver segment I, and there is a lack of a general field of view during the procedure. In the CT-guided technique, the image can display a comprehensive distribution of all liver lesions, and CT is sensitive for identifying the occurrence of complications, such as pneumothorax, in a timely manner. However, some unavoidable changes in posture and breath movement may affect the actual puncture accuracy, causing it to deviate from the prescribed puncture plan. Therefore, it may be necessary to repeat needle insertion adjustments, with implications for radiation accumulation during each scan and contrast agent nephrotoxicity. There are also some differences between these two imaging modalities in terms of identifying smaller lesions [7], differentiating complex cystic lesions in particular [8], and evaluating the outcomes of treatment [9], which are important aspects of treatment strategy, efficacy, and prognosis. Although these modalities have been widely applied in ablation, the results of previous studies were based on comparisons between the ablation itself and combination treatments. Few reports have investigated treatment-related factors and outcomes between the two imaging modalities in CLOM patients. High-level evidence to provide a basis for decision-making is scarce, and additional evidence from a real-world setting is also required. The purpose of this study was therefore to review these two imaging guidance techniques within a set of patients and analyze the factors associated with the outcomes of their initial ablation treatments.
Materials and Methods
Compliance with Ethical Standards
This retrospective study was approved by the ethics committee of the authors’ affiliated center (IRB: GZR2018-143), and a consent waiver was obtained. All procedures performed in this study were in accordance with the Declaration of Helsinki and its later amendments or similar ethical standards.
Patient Selection and Data Collection
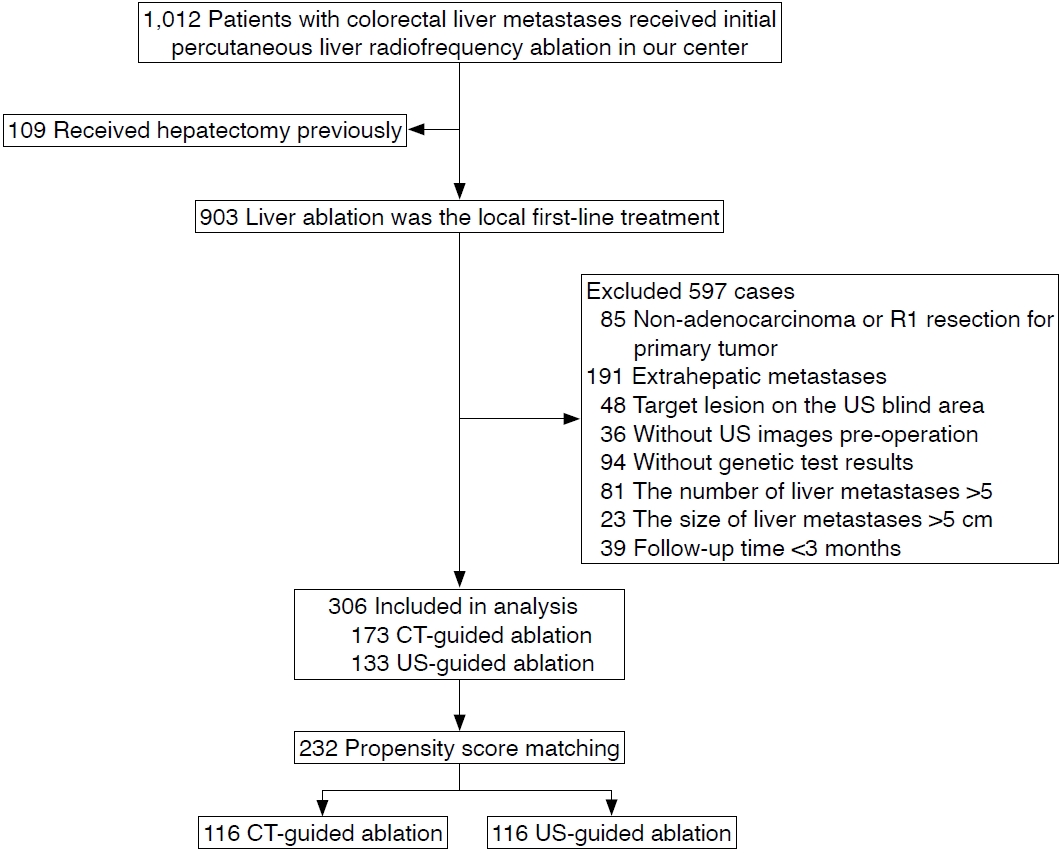
Patients diagnosed with colorectal liver metastases between January 2008 and January 2021 were retrospectively reviewed. The inclusion criterion for analysis was that percutaneous liver RFA was the initial treatment at the authors’ affiliated center, without previous liver ablation. The exclusion criteria were as follows: (1) previous hepatectomy; (2) non-adenocarcinoma or R1 resection for the primary tumor; (3) extrahepatic metastases at initial treatment; (4) the availability of only CT or US pre-procedure images, or lesions with poor sonic vision on US; (5) unavailable genetic test results; (6) >5 liver metastases or liver metastases >5 cm in size on CT or magnetic resonance imaging enhancement (for patients who received chemotherapy before ablation, liver metastases were limited to ≤5 after completing the last cycle of chemotherapy); and (7) follow-up time <3 months. A detailed flowchart of patient selection is shown in Fig. 1.
Ablation Treatment
After administration of intravenous and local anesthesia, RFA was performed under real-time US (MyLab 90, Esaote SpA, Firenze, Italy) or CT (Siemens, Munich, Germany) guidance by two teams of interventional oncologists with three doctors in each group who had 7-20 years of experience in US-guided ablation or CT-guided ablation. The decision between CT and US guidance was made by multidisciplinary team conferences after fully informing the patients about the procedures in detail and obtaining informed consent.
Before ablation, for poorly visualized or ill-defined lesions, contrast enhancement was employed to detect the target lesion more clearly. The US contrast agent was SonoVue (Bracco, Milan, Italy), supplied as a lyophilized powder and dissolved in 5 mL of saline solution to form a homogeneous microbubble suspension. The CT contrast agent was Omnipaque.
A radiofrequency system (RF 2000, RadioTherapeutics, Mountain View, CA, USA) and a needle electrode with a 15-G insulated cannula with 10 hook-shaped expandable electrode tines with a 3.5-cm diameter at expansion (LeVeen, RadioTherapeutics, Natick, MA, USA) were used. After the electrode was inserted into the center of the tumor, the radiofrequency generator was activated and initiated with a power of 10 W, and its intensity was increased at a rate of 10 W/min, with a mean power of 110 W (40-200 W) during each application. No more than three electrodes were used in a procedure. For tumors with a size ≤3.0 cm, a single electrode was inserted. For tumors with a size >3.0 cm, multiple electrodes were inserted. The distance between two electrodes was about 1.0-1.5 cm.
Strategies concerning the optimal ablation process and evaluation of technical success were discussed and confirmed in an ablation team meeting. After ablation, contrast-enhanced CT (CECT) or US (CEUS), matching the former guidance modality, respectively, was immediately performed. Complete ablation was defined as devascularization of the lesion without an enhancing area within the ablation zone on CEUS or CECT [10]. Supplementary ablation was performed when a residual area of a viable tumor or suspicious lesion was identified by real-time detection. For technical success, the target lesion had to be covered entirely by the echogenic zone on US (in an orthogonal view) or the ablation zone on CT when completing treatment. The ablative margin was assessed 1 month after ablation on CECT by two board-certified operator members in the team mentioned above in a consensus manner. Pre-and post-RFA CECT images were displayed side by side. Anatomic landmarks around the lesion were chosen, and the distance from the edge of the lesion to the landmarks was measured. For each landmark, the pre-RFA distance was subtracted from the post-RFA distance, yielding the value at that site, and the shortest value was designated as the minimal ablative margin [11]. For follow-up, scheduled triple-phase CECT was performed for evaluation 1 month after the initial discharge and every 3 months thereafter.
The procedure time was defined as the duration from the start of local anesthesia before the ablation puncture until the patient left the procedure room. The cost was defined as treatment-related expenses beginning from the ablation procedure until hospital discharge, including the cost of ablation appliances and complication treatment, priced in US dollars.
The specific tumor location was classified as perivascular (tumor with any contact with a first- or second-degree branch of portal or hepatic vein that was ≥3 mm in distance) and subcapsular (when the nearest distance from the liver capsule to the tumor margin was <10 mm) on axial or coronal CT [12,13]. Otherwise, the tumor location was treated as unspecific.
Follow-up Definition
The follow-up period was the duration from the date of ablation until death or the last visit up to July 1, 2021. Local tumor progression (LTP) was defined as any new peripheral or nodular enhancement within 1 cm outside the area of the previously treated site [11].
The initial ablation treatment was used in the present analysis. The primary endpoint was LTP-free survival (defined as the duration from the date of ablation to the first radiographic evidence of LTP). Overall survival (OS) was the duration from the date of ablation to the date of death or the last visit in this study. Complications were classified according to the Society of Interventional Radiology guidelines as minor (having no consequences and requiring no therapy) or major (requiring therapy and hospitalization) [14]. The LTP-free survival, OS, treatment time, costs, and complications were compared between the two groups.
Statistical Analysis
To balance the baseline data before analysis, propensity score matching (PSM) was used and estimated by a logistic regression model. The variables included in the PSM were: age, sex, comorbidities, primary tumor location, T category, N category, differentiation, KRAS status, carcinoembryonic antigen (CEA) levels, diameter, number of metastases, synchronous or metachronous liver metastases, and chemotherapy before ablation. The matching ratio between the two groups was 1:1 using the nearest-neighbor matching method (caliper=0.1). To assess the balance of variables used for matching, we applied the standardized mean difference to determine whether values were lower than 0.1.
All statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA) and GraphPad Prism version 7.0 (GraphPad LLC, San Diego, CA, USA). Unless otherwise specified, data related to survival outcomes were expressed as median (range), and other data were presented as mean±standard deviation. The results were compared using the Student t-test, chi-square test, or Fisher exact test as appropriate. We calculated the LTP-free survival and OS using the Kaplan-Meier method and compared them using the log-rank test. Any factors that showed clinical significance for LTP according to the univariable analysis were further entered into a multivariable Cox proportional hazard model. A P-value <0.05 (two-sided) was considered to indicate statistical significance.
Results
Ablation Characteristics
Ablation was performed in 507 lesions in 232 patients (269 and 238 lesions in the US-guided and CT-guided group, respectively), and the mean number of ablated lesions per patient was 2.19±1.41. The liver segment distribution of lesions is shown in Table 3; 72 and 62 lesions had a perivascular location in the two groups, respectively, while 42 and 45, respectively, showed a subcapsular location.
The mean procedure time in the US-guided group was less than that in the CT-guided group (27.54±12.06 minutes vs. 32.70±13.88 minutes, P=0.003). In the cost analysis, the mean expense was $2,175.13±618.17 in the US-guided group and $2,455.49±710.25 in the CT-guided group (P=0.002) (Table 4).
LTP-Related Outcomes and Subgroup Analysis
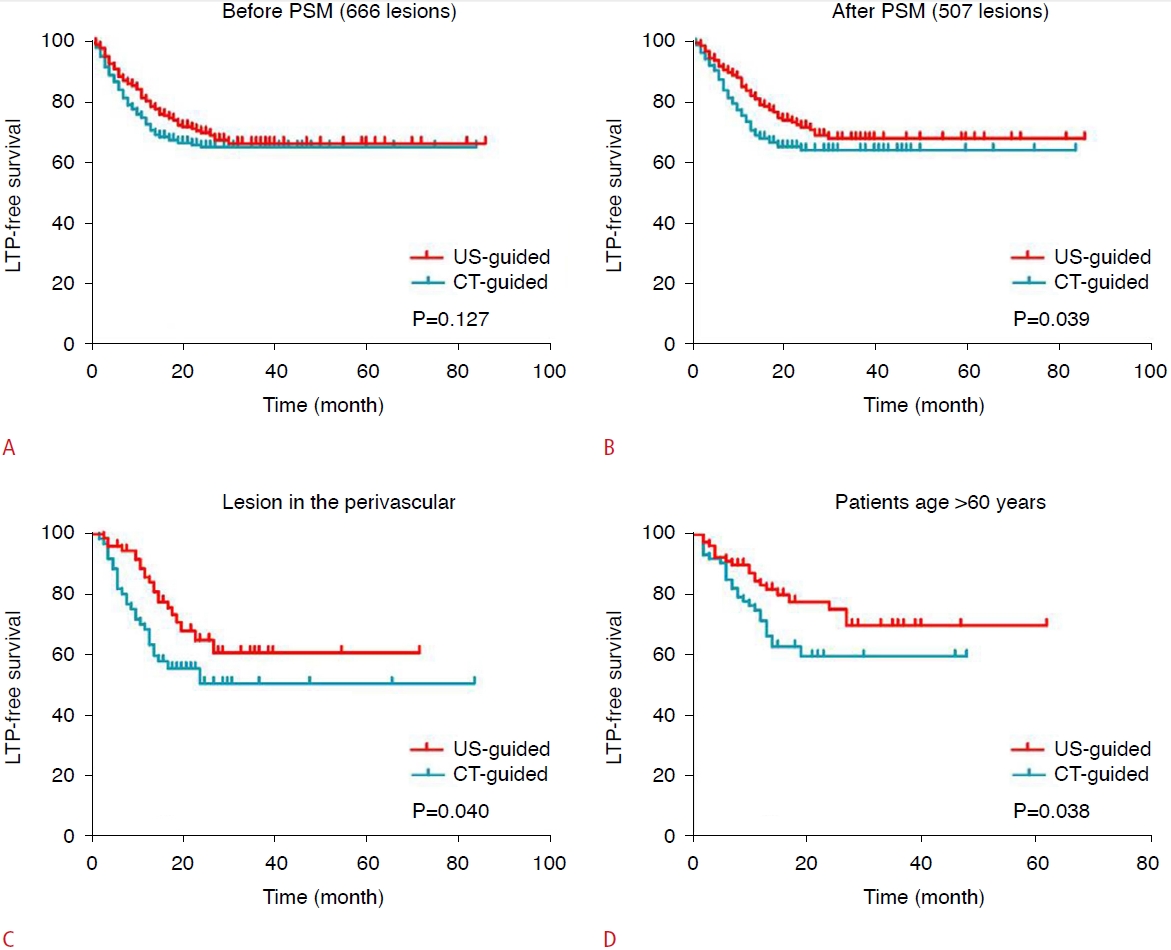
Before PSM, the total cumulative LTP rates at 1, 3, and 5 years were estimated as 21.8%, 34.1%, and 34.1%. The cumulative LTP rates at 1, 3, and 5 years were 18.3%, 33.4%, and 33.4% in the US-guided group and 24.0%, 34.7%, and 34.7% in the CTguided group, respectively (P=0.127) (Fig. 2A). After PSM, the total cumulative LTP rates at 1, 3, and 5 years were 19.2%, 33.9%, and 33.9%, and the cumulative LTP rates at 1, 3, and 5 years were 15.9%, 31.9%, and 31.9% in the US-guided group and 24.2%, 35.7%, and 35.7% in the CT-guided group, respectively (P=0.039) (Fig. 2B). The median OS after PSM was 65.00±10.40 months (5-110 months) and 53.00±7.76 months (4-105 months) in the two groups, respectively (P=0.666).
For perivascular lesions, the cumulative LTP rate at 1 year was 14.4% in the US-guided group and 28.2% in the CT-guided group (P=0.040) (Fig. 2C); for subcapsular lesions, there was no statistically significant difference between the two groups (P=0.444), with a 1-year cumulative LTP rate of 15.8% in the US-guided group and 22.5% in the CT-guided group. For patients >60 years of age, the cumulative LTP rate at 1 year in the US-guided group was 17.8% and that in the CT-guided group was 25.1% (P=0.038) (Fig. 2D).
Univariable and multivariable analyses for LTP are shown in Table 5. In the multivariable analysis, lesion diameter >3 cm (hazard ratio [HR], 1.580; P=0.018), ablation margin <5 mm (HR, 0.453; P=0.002) and the presence of a KRAS mutation (HR, 1.860; P=0.001) were identified as independent predictors of LTP.
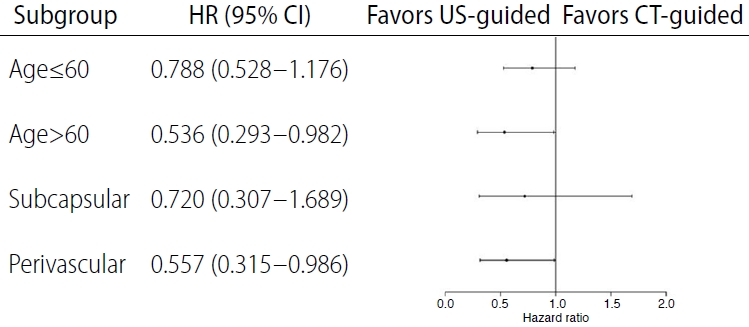
A forest plot analysis of factors for US-guided ablation is shown in Fig. 3, including age >60 years and perivascular liver lesions.
Complications
No treatment-related deaths occurred during the ablation procedures, and the total incidence of complications was 9.9% (Table 4). These complications were managed as appropriate by means of chest tube placement, drainage, anticoagulation, intravenous antibiotics, and fasting.
Discussion
The patients analyzed in the final cohort were those who had both CT and US pre-procedure images, and their lesions were visualized on non-contrast or contrast enhancement imaging. Park et al. evaluated the therapeutic effectiveness of CT-guided RFA in a hepatocellular carcinoma (HCC) cohort. However, the lesions in their study were undetectable on US images [15]. Huo et al. [16] performed another comparative study, but they focused on a cost comparison between CT-guided and US-guided ablation. The total cumulative LTP rate at 1, 3, and 5 years in this study were within the outcome range reported in other similar studies [11,13,17]. The majority of LTP occurred in the first 3 years in this study, which is also in line with the findings of these prior studies [11,13].
The cumulative LTP rate in the US-guided group was lower than that in the CT-guided group, which could be explained by reasons including but not limited to the following. First, real-time observations were made with visualized punctures and higher accuracy during percutaneous interventions under US guidance, which meant that an invalid needle track occurred less frequently [18]. In most cases, there was one needle track under US-guided ablation because of the real-time visualization ability and adjustment. Thus, the needle track could be ablated along with the needle direction before each needle adjustment. However, for CT-guided ablation, it was possible that more than one needle track or direction existed because repeat needle adjustment was finished in each discontinued scan under semi-blinded punctures without real-time monitoring. Although the lesion around the needle was ablated, it is possible that some micro-lesions metastasized along the previous needle track or the injured intra-hepatic vessels adjacent to the tumors [19]. Second, electrode placement, which is a prerequisite factor for ablation, under US guidance might be more centered or "suitable" within the target lesion than CT guidance, covering the whole lesion more sufficiently with overlapping ablation areas [20]. Third, the partial volume effect, slice thickness, or metal artifacts on CT might interfere with the determination of tiny lesion residue. Peripheral rim enhancement after RFA might mask some small residual tumors [21]. Fourth, the evaluation of the ablation area on CT might be imperfect if it is not performed by a three-dimensional assessment, which can be limited by the misalignment of the liver due to patient’s position, respiratory phase, tissue attenuation changes after ablation, or image resolution [20,22,23]. The hyperechoic halo around the ablation area on US with real-time and flexible orthogonal planes and the use of a contrast agent could increase conspicuousness and make the extent more clearly and reliably identifiable [24,25]. However, the hyperechoic region during ablation (before it gradually diminishes) is an interference factor that can present irregular contours and obscure the tumor and electrode, potentially increasing the difficulty of ablation [26,27]. Fifth, some small cystic liver metastases can be effectively detected and differentiated by dynamic CEUS [28,29], especially in patients who show a good response to neoadjuvant chemotherapy. These small and highly suspicious lesions could have been ablated, and local disease control improved. Therefore, from the standpoint of technique and imaging, US might potentially lead to more reliable ablation in some cases. More studies assessing which modality is optimal for liver image-guidance ablation among these patients are expected.
We found that patients >60 years of age were suitable for US-guided ablation. A possible reason is that breath coordination is simpler when using US than when using CT in older patients due to the fact that their hearing conditions and breath-holding actions might be poorer compared to younger patients. Perivascular lesions, especially in large vessels, are known to be difficult to treat. Although increasing the power or time when performing perivascular ablation is helpful, placing the electrode as parallel or close as possible to the vessels to increase the contact surface with the large vessel [30,31] seems to be particularly important, and it is safer and easier to achieve this goal under US real-time guidance.
US is an ideal guidance and targeting modality in experienced hands because of its inexpensive, fast, and safe contrast agent for patients with insufficient renal function. An HCC study compared complications between CT-guided and US-guided ablation, including four and two cases of abdominal bleeding in the two groups, respectively [32]. There were seven cases of pneumothorax, three cases of bleeding, and one case of liver abscess in the CT-guided group. These were primarily induced by repeated needle adjustment that injured the pleura, the liver capsule, or the vasculature due to poor breath cooperation during the puncture. Spending more time on needle adjustment prolongs the procedure and increases the incidence of complications. Compared to real-time observations for US, needle adjustment for CT guidance was more time-consuming due to repeated scans, and breath movement affected the insertion accuracy at each discontinued puncture, leading to readjustment. More studies are needed to validate and summarize the relationship between image guidance modalities and the occurrence of complications.
The procedure duration and expense for ablation treatment in the US-guided group were less than those in the CT-guided group. An HCC cohort supported the claim that US-guided ablation was cost-efficient in comparison to CT-guided ablation (mean cost, $1,862±1,352 and $2,847±1,690, respectively; P<0.001) with similar efficacy [16]. With the incidence of cancerous disease increasing over the past decade and the utilization of ablation becoming more frequent, a balance needs to be reached between treatment efficacy, safety, and expense [33]. The concept of "less is more" deserves consideration [34].
The present study had some limitations. First, this was a retrospective study from one center, making it necessary to validate the findings through more studies in the future. Although the baseline data were more balanced after PSM, some patients were excluded from the final analysis, impairing the raw data. Second, the evaluation of complete ablation by CT and US is different. Therefore, establishing a reliable and objective method of intraprocedural assessment warrants further investigation. Third, there was no further investigation of re-ablation treatment for recurrent lesions. The intention of the present study was to compare the two image guidance modalities separately rather than in combination because one goal of this study was to provide objective results and theoretical support for wider application of the fusion imaging technique. Thus, further studies on fusion imaging ablation are warranted in subsequent work. Fourth, the KRAS test results came from sampled primary tumor tissue. Although Loes et al. [35] found that the genotype in colorectal cancer exhibited mutation heterogeneity between metastatic and primary lesion tissues. Knijn et al. [36] and Voutsina et al. [37] showed that the genotype of metastatic lesions was highly consistent with that of primary tumor samples. Thus, the present study performed a KRAS analysis based on the status of primary tumor tissue. Fifth, liver lesions were diagnosed according to CEA levels and pre-procedure images, meaning that there was a lack of pathological evaluation of the target lesions before and after ablation. This evaluation would have been important, as such an examination might have provided information about the risk for tumor progression and biological behavior [38,39].
In conclusion, when patients are over 60 years of age or have perivascular liver lesions, US-guided ablation is better than CT-guided ablation, with a shorter treatment time and lower costs for patients in whom both ablation methods are feasible. More studies are needed to validate our findings.
 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI



