

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
In high-income countries, endometrial cancer is the most common gynecological malignancy, including 4% of all female cancers worldwide [1,2]. Moreover, the prevalence of endometrial cancer is expected to increase in the near future [3]. Women from low-income and middle-income countries are significantly more likely to die from endometrial cancer than those from high-income countries, reflecting poor access to adequate resources [1,2]. Surgery is the primary staging and treatment approach for early endometrial cancer [3]. Lymphadenectomy is required for surgical staging in endometrial cancer; however, it does not offer a survival advantage and is associated with an increased surgical burden [4,5]. An accurate and cost-effective presurgical workup can improve the treatment quality, reducing the frequency of overtreatment or undertreatment and enabling broader access to appropriate staging in resource-limited settings.
For several years, staging ultrasonography in endometrial cancer has proven to be a valid and reproducible method [5–7]. Expert ultrasonography and magnetic resonance imaging (MRI) are both critical in the diagnostic workup of endometrial cancer for local tumor extension [5,7]. Models based on ultrasound staging have also been proposed to predict lymph node involvement [4]. Local tumor extension and the prediction of lymph node involvement influence the patient’s management [4,5]. These results direct the surgical management in terms of whether to perform systematic lymph node dissection or lymph node biopsy assessment [4,5]. Moreover, imaging can serve as a decision instrument for further management in women with failed sentinel lymph node biopsy [4].
Evaluating the learning curve (LC) in a structured program is useful for standardizing medical procedures [8–10]. Similar studies have been proposed in gynecological ultrasound examinations for other conditions, such as ovarian cancer, endometriosis, or congenital uterine anomalies [8–10].
Completing an advised number of ultrasound examinations is the typical approach for professional training in ultrasound imaging. However, this method lacks objective evidence regarding individual competency. Statistical methods have been applied to analyze interventional and diagnostic LCs to overcome this issue. The cumulative summation (CUSUM) test and the LC-CUSUM test have been used multiple times for this purpose [9,11–13]. However, to the best of the authors’ knowledge, the LC-CUSUM test has not yet been well characterized in the ultrasound staging of endometrial cancer.
Therefore, this study aimed to use the LC-CUSUM test to assess the skill acquisition process for performing ultrasound staging of endometrial cancer.
Materials and Methods
Compliance with Ethical Standards
In this retrospectively designed study, data were collected after reviewing medical records during the 2017-2019 period at Santa Maria della Misericordia University Hospital (a tertiary referral center). This investigation was carried out with internal review board approval, following the Helsinki Declaration, and according to local data protection authority dictates (number 049/2021). The need for informed consent, according to national legislation, was waived by the IRB listed above because this was a retrospective study.
Setting and Sample
The study was conducted at a tertiary academic hospital with a reference population of more than 500,000 inhabitants and an annual average of 35,000 hospitalizations. Endometrial cancer patients were routinely managed during the study period according to the local guidelines [14]. During the same period, beyond MRI and the computed tomography imaging, an advanced ultrasonography examination was also introduced to map the disease extension preoperatively. This ultrasound examination was recorded in the hospitalization files and used by the surgeons as additional information during the surgical procedure. From the inception of the preoperative ultrasound examinations to April 2019, data on the ultrasound staging, intraoperative assessment, and final pathology report were collected. All consecutive eligible patients were included. The exclusion criteria included the absence of ultrasound data and patients not undergoing surgery after the preoperative workup.
Data Collection and Measurement
Clinical data were recorded on a standard spreadsheet. The data contained patient demographics, ultrasound examinations, surgical reports, and definitive pathology data. The following outcomes were considered: myometrial invasion, uterus serosa invasion, pelvic lymph nodes positivity, and para-aortic lymph nodes positivity. The success or failure of the ultrasound examination assessment was established according to the intraoperative exploration and the definitive pathology report.
The extent of myometrial tumor invasion was evaluated using the Karlsson ratio [15]. The degree of infiltration into the myometrium was determined by measuring the anteroposterior diameter of the tumor (d1) and relating it to the anteroposterior diameter of the uterus (d2) in the sagittal plane [15]. In detail, if the ratio of d1 to d2 is <50%, myometrial invasion was estimated as less than half of the myometrium (stage 1a); in contrast, if the ratio is >50%, it was classified as more than half of the myometrium (stage 1b) [15]. Interruption of the hyperechoic line surrounding the uterus serosa by the tumor infiltrating the myometrium wall was considered as serosal involvement. Lymph nodes were examined principally by transabdominal sonography using a convex-array probe [16,17]. The standard approach started from the inguinal to iliac and para-aortic nodes. The inguinal lymph nodes are situated caudally to the level of the inguinal ligament. Once the inguinal lymph nodes were assessed, the probe was placed in an oblique section to evaluate the external vessels located on the psoas major muscle. The obturator fossa is under the external iliac vessels, and at the pelvic margin it follows the bifurcation of the internal and external iliac vessels. The examination continued with an evaluation of the common iliac vessels and periaortic and peri-caval vessels. The sagittal plane was obtained to check these nodes and move from the aortic/caval bifurcation to the diaphragm. The probe was placed from left to right and back by small movements during the entire course of the aorta and cava [16,17].
In all cases, the examiners used both approaches, with transvaginal and transabdominal probes, as part of the standard methodology for staging endometrial cancer. Transvaginal ultrasonography was used to assess the pelvic organs and myometrial invasion, while transabdominal ultrasonography was used to evaluate the inguinal, iliac, and para-aortic lymph nodes [16,17].
Both operators were experienced ultrasonographers (more than 5 years of experience in ultrasonography) blinded to the other imaging results, and the pathologist was blinded to the ultrasound examination results. All the ultrasound examinations were performed with a Voluson E10 General Electric (General Electric Medical Systems, Zipf, Austria) or a Voluson E6 (General Electric Medical Systems) instrument. All investigations were performed with a high-resolution ultrasound transabdominal probe (2-8 MHz convex transducer) or a high-resolution ultrasound transvaginal probe (5–9 MHz transducer) (General Electric Medical Systems). All the ultrasound probes had three-dimensional capabilities.
Data Analysis
The LC-CUSUM test was designed to inform when the operator performance is sufficiently far away from an unsatisfactory performance level to evaluate the performance as acceptable [11,13]. It supposes that a newcomer operator is not performing adequately at the start of monitoring. Afterward, it reports when the operator achieves a satisfactory level of performance [13,18]. Unlike LC-CUSUM, the CUSUM test is designed for monitoring the transition from an adequate to an inadequate performance level, and it can be used after LC-CUSUM to monitor whether the performance is maintained within an acceptable range [13]. Acceptable and unacceptable rates were designated according to the previously published literature [9]. For the LC-CUSUM test, the null hypothesis was set at a failure rate of 25% (suboptimal implementation), while the alternative hypothesis was set at a failure rate of 10% (optimal implementation) [9]. For the CUSUM test, the null hypothesis was set at a failure rate of 10% (optimal implementation), while the alternative hypothesis was set at a failure rate of 25% (suboptimal implementation) [9]. The accepted type I and II errors of 0.1 and 0.1, respectively, entailed a limit of h=2.0 for both curves [9].
All statistical analyses were executed with R software (version 3.6.3, R Core Team 2020, R: A language and environment for statistical computing; R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org/). Continuous variables are shown as the median and interquartile range (IQR) or mean and standard deviation. Dichotomous variables are shown as frequencies (%) and absolute values, and missing values were excluded from the analysis. Furthermore, sensitivity, specificity, and accuracy were analyzed and presented with their 95% confidence intervals.
Results
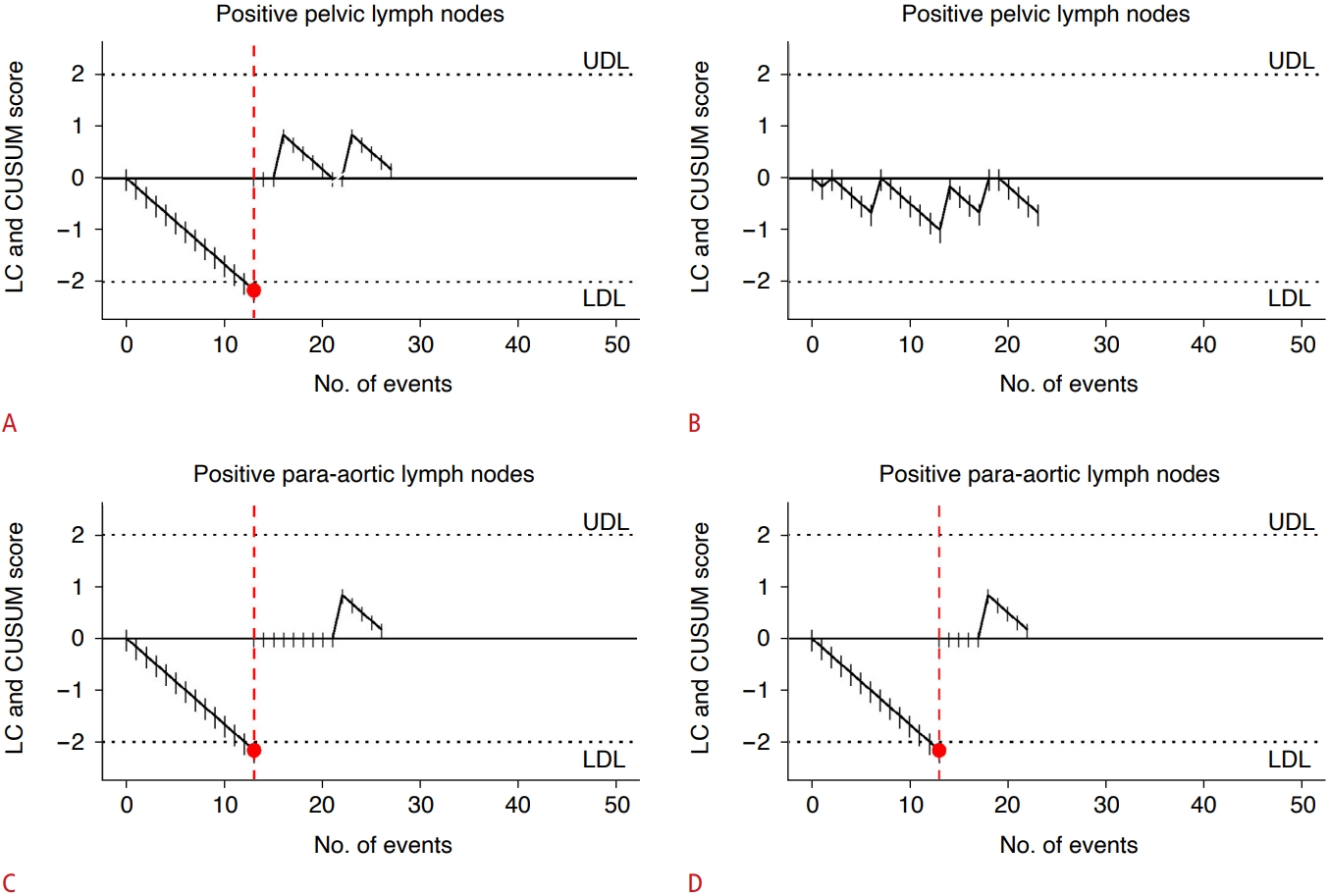
The two operators performed 67 procedures during the study period. Table 1 shows the detailed numbers of ultrasound examinations eligible for inclusion per site. The number of procedures required to achieve competence is reported in Table 1. Operator 1 performed 42 procedures for the myometrial invasion diagnosis, and the number required to achieve competence (NRTAC) according to LC-CUSUM was 29 (Table 1, Fig. 1A). Operator 2 had only a limited number of procedures, and it was not possible to establish the NRTAC (Fig. 1B). For serosa invasion, operator 1 had an NRTAC of 39 and operator 2 of 13, with a mean value of 26 procedures (Table 1, Fig. 1C). For pelvic lymph nodes assessment, the NRTAC was only calculated for operator 1, resulting in 13 procedures (Table 1, Fig. 2A). Operator 2 did not reach the limit to calculate the NRTAC (Fig. 2B). The NRTAC was 13 procedures in both operators to diagnose positive paraaortic lymph nodes (Table 1, Fig. 2C, D).
Discussion
The present study tested the implementation of a new diagnostic pathway in the presurgical workup of endometrial cancer using LC-CUSUM, which represents a tailored approach to individual learning. The processes reached satisfactory performance in the majority of the cases according to the established definitions. Moreover, the ultrasound staging for endometrial cancer was highly accurate.
This study demonstrated the feasibility of using the LC-CUSUM test to assess the performance for auditing the introduction of a presurgical staging pathway to the traditional management. Satisfactory performance was achieved by operator 1 within the first 67 subjects examined, and moreover, the performance was maintained according to the established definitions. The second operator performed fewer procedures and did not achieve adequate performance in all the predefined outcomes at the audit time. Previous studies on gynecological ultrasonography adopted the LC-CUSUM method to assess the efficacy of a predetermined training program [8–10]. Those previous studies all highlighted the satisfactory use of the LC-CUSUM test to assess progress and monitor the skills achieved by the trainees [8–10].
The ultrasound staging of endometrial cancer is a hot topic. Ultrasound imaging is a simple and affordable methodology that has several advantages [17]. This technique is increasingly supported for the staging of endometrial cancer [5,19]. In the literature, the sensitivity of ultrasound imaging for assessing myometrial invasion ranges between 70% and 100% and the specificity between 70% and 90% [19–21]. In addition, the sensitivity and specificity of the subjective assessment of cervical stromal invasion range from 25% to 93% and from 85% to 99%, respectively [22,23]. Different studies and a recent meta-analysis comparing MRI and ultrasonography did not highlight any significant differences between the accuracy of the two methods [21,24–26]. The only thing that stands out is the more substantial variability in the accuracy of the ultrasound scans, probably because ultrasonography is a more subjective technique or simply because of improvements in the equipment available in recent years [21]. Moreover, recent studies have proposed less subjective and more standardized methods to assess myometrial invasion in endometrial cancer, showing an improvement in diagnostic accuracy [5,19]. The data of the present study showed an overall accuracy overlapping with previously published literature [5,20].
Some possible limitations of this study should be noted. First, the LC-CUSUM test was employed by a small number of operators for a relatively limited number of women affected by endometrial cancer. Thus datasets with other numbers and different working conditions might show dissimilar results. However, even with this limitation, the LC-CUSUM test showed its potential value for monitoring the introduction and the continuation of a new diagnostic pathway, ensuring adequate quality achievement and quality maintenance. Second, this is a retrospective study with all the limitations of a retrospective design. Future studies should consider a prospective design with a predefined protocol to avoid any possible bias innate in the retrospective design.
This study investigated the usefulness of applying the LC-CUSUM test to endometrial cancer ultrasound staging. The data showed the utility of the LC-CUSUM method for monitoring the LC and preserving adequate standards.

 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI



