

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Radiofrequency ablation (RFA) is used to treat benign thyroid nodules and thyroid cancers, and many studies have demonstrated its efficacy and safety [1,2]. However, several long-term follow-up studies have reported a tendency for marginal regrowth after 2 to 3 years of follow-up [3-5]. Therefore, repeated RFA is often required for nodules showing marginal regrowth [3]. To prevent marginal regrowth, it is crucial to achieve complete ablation of the nodule, including the margins, while minimizing the amount of residual tissue [6,7]. To achieve more complete ablation, two types of vascular ablation techniques have been proposed: the artery-first ablation technique and the marginal venous ablation technique [8,9].
Of these two vascular ablation techniques, the venous ablation technique directly ablates the marginal draining veins. Ablation of these marginal draining veins is useful for complete ablation of the nodule margin, thereby preventing marginal regrowth [3,9]. However, it is technically difficult to ablate the margin of the nodule completely because of pain. In addition, there is a greater risk of complications when the nodule tissue is close to a critical structure, such as medial type vagus nerves and medial type sympathetic ganglia, as well as in cases of anatomic variations of the recurrent laryngeal nerve. To overcome these difficulties, it is helpful to use the hydrodissection technique with 5% cold dextrose solution [10,11].
The hydrodissection technique involves creating a sufficient safety margin by injecting a solution around the thyroid capsule to separate the target ablation area from adjacent critical structures. Various hydrodissection techniques and four different approaches can be used (the anterolateral, posterior, pre-tracheal, and danger triangle approaches), with the choice depending on the tumor location [12]. For several years, the thyroid ablation team at the authors’ affiliated institution has routinely used the anterolateral hydrodissection (ALHD) technique to safely facilitate venous ablation and prevent marginal regrowth of benign thyroid nodules. This study presents the authors’ experience of ALHD for the ablation of benign thyroid nodules, introducing the preliminary cases using the ALHD technique and evaluating its technical feasibility, efficacy, and safety during RFA of benign thyroid nodules.
Materials and Methods
Compliance with Ethical Standards
This retrospective study was approved by the institutional review board (2021-1452) of Asan Medical Center. The requirement for written informed patient consent was waived because of the retrospective nature of the study.
Patient Selection
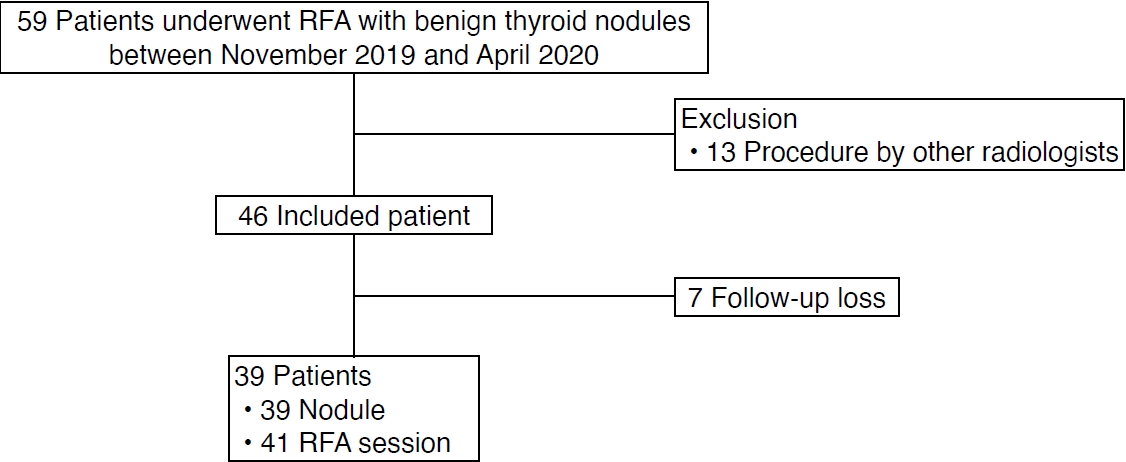
Between November 2019 and April 2020, 59 patients underwent RFA for biopsy-proven benign thyroid nodules causing cosmetic or symptomatic problems (Fig. 1). Thirteen patients who were treated with RFA by radiologists other than J.H.B. were excluded. Seven patients who were lost to follow-up before 6 months were also excluded. Finally, 39 patients with 39 benign thyroid nodules who underwent a total of 41 RFA sessions were included in this study. All procedures in the included cases were performed by an experienced radiologist (J.H.B. with 26 years of clinical experience in performing the procedure).
Pre-procedural Assessment
Ultrasound examinations were performed using ATL HDI 5000, iU22 (Philips Healthcare, Best, The Netherlands), or RS 80 (Samsung Medison Co., Ltd., Seoul, Korea) systems. Each system was equipped with a linear high-frequency probe (5-14 MHz). All ultrasound examinations and ultrasound-guided core needle biopsies were performed under the supervision of staff radiologists with at least 11 years of clinical experience in performing and evaluating thyroid ultrasound images.
Three orthogonal diameters were measured, and the volume of each nodule was calculated. The nodule composition was graded into four categories according to the proportion of the solid component: grade 1, solid with no obvious cystic content; grade 2, predominantly solid with a cystic content ≤50%; grade 3, predominantly cystic with a cystic content >50%; and grade 4, cystic with no obvious solid content [13]. Nodule vascularity was graded into four categories on the basis of a Doppler examination: type 1, no intra-nodular vascularity; type 2, peri-nodular vascularity only; type 3, intra-nodular vascularity <50%; and type 4, intra-nodular vascularity >50% [13].
Before RFA, the physician recorded a cosmetic score as follows: 1, no palpable mass; 2, no cosmetic problem but a palpable mass; 3, cosmetic problem on swallowing only; and 4, readily and always detected cosmetic problem. Baseline patient-determined symptom scores were rated using a visual analogue scale from 0 to 10 [14].
RFA Procedure and ALHD Technique
RFA was performed according to the guidelines of the Korean Society of Thyroid Radiology [14]. RFA was performed using a radiofrequency generator (VIVA RF generator, STARmed, Goyang, Korea; M-2004, RF Medical, Seoul, Korea) and 18-gauge thyroid-dedicated modified internally-cooled electrodes (VIVA, STARmed; RFT-0710, RF Medical) with various active tip sizes. The size of the active tip (5, 7, and 10 mm) was selected according to the size of the thyroid lesion.
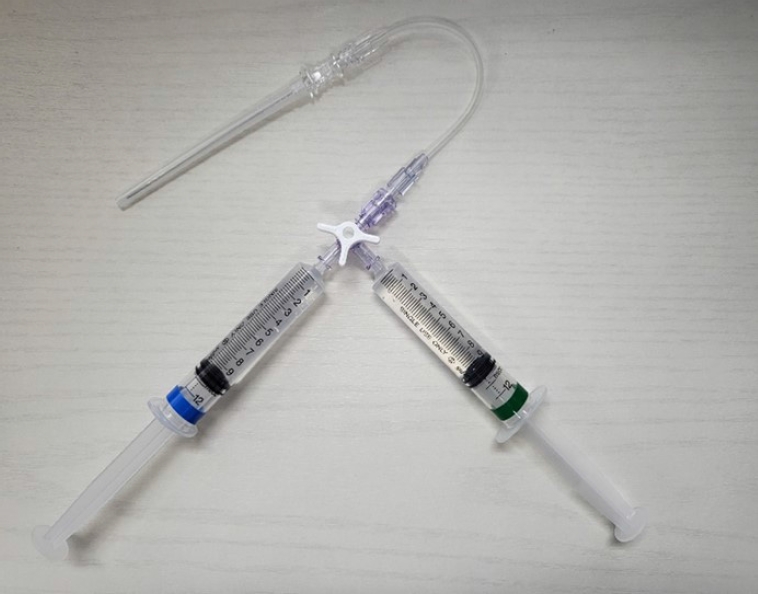
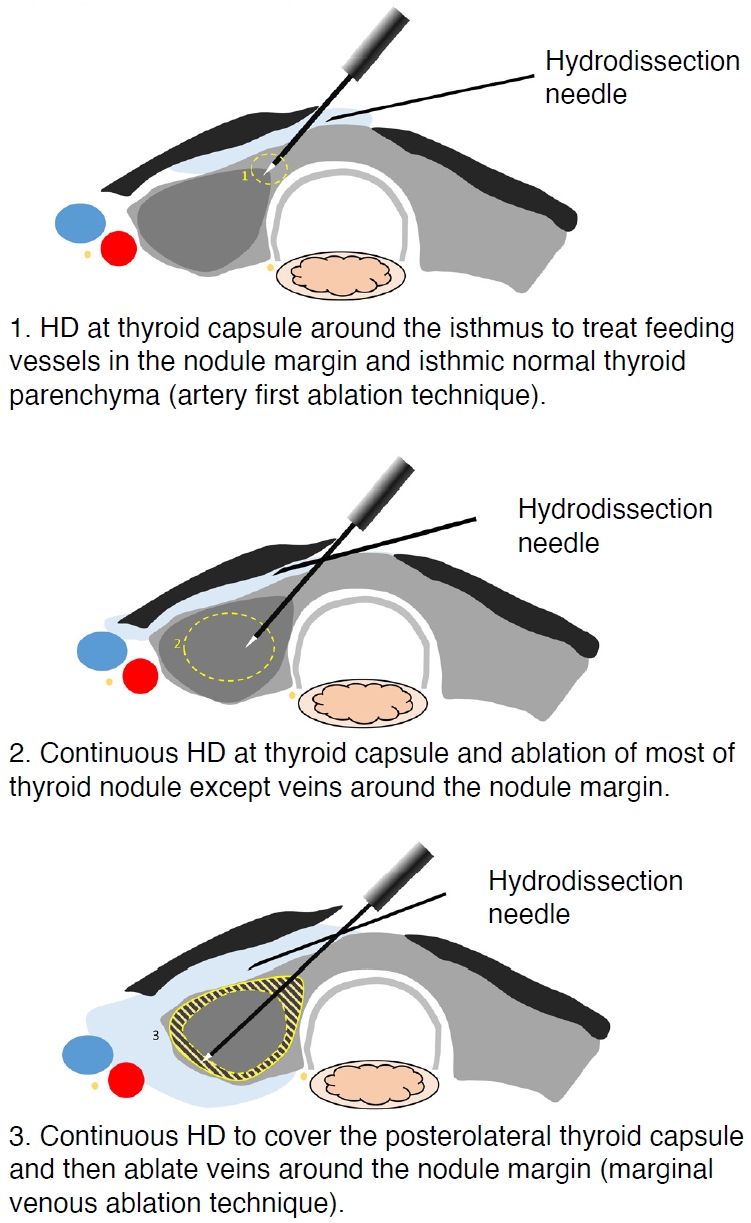
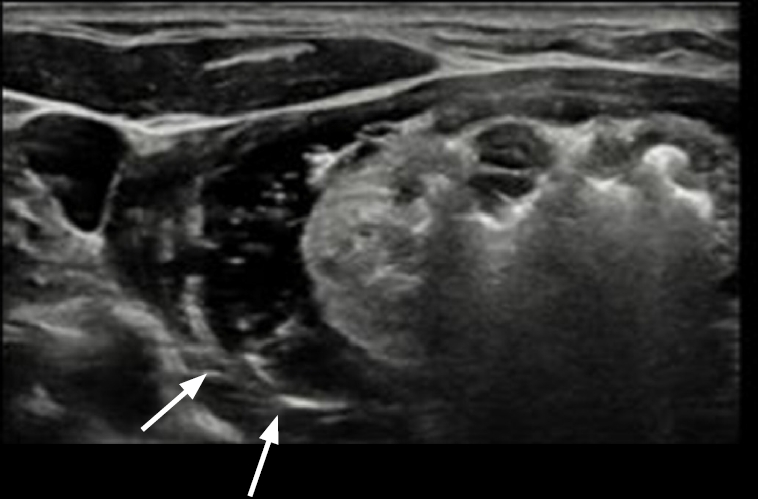
The ALHD technique was routinely used for RFA of benign thyroid nodules. A 21G spinal needle with a three-way stopcock was used for both local anesthesia and ALHD with a single skin puncture site (Fig. 2). The overall procedure of ALHD with RFA is illustrated in Fig. 3. First, for local anesthesia, a lidocaine needle was inserted at the midline of the anterior neck, just above the thyroid isthmus, and advanced into the thyroid capsule. The patient was injected with 1% lidocaine at the skin puncture site and the perithyroidal area including the strap muscle and thyroid capsule. Next, RFA of the benign thyroid nodule was started. RFA was performed using the trans-isthmic approach and the moving-shot technique, and the ALHD technique was routinely applied during the RFA procedure. We approached the target nodule by dividing it into three portions and ablating them in the following order. First, the most anteromedial portion of the nodule near the isthmus was targeted for ablation. Second, the central portion of the nodule was targeted. Lastly, the peripheral portion of the nodule, which was relatively close to critical perithyroidal structures, was targeted with hydrodissection. If the patient complained of pain during ablation of the nodule margin, additional ALHD was performed (instead of using more local anesthesia) with cold (0°C to 4°C) 5% dextrose solution to control the pain and secure sufficient safety margins from critical structures (Fig. 4). Injection of fluid and constant monitoring of the relationships between the nodule and critical structures including nerves, esophagus, and pain-sensitive structures such as the strap muscle and skin were required. The distance between the thyroid gland and strap muscle was maintained at more than 5 mm. RFA was terminated when the entire targeted lesion was covered with hyperechoic microbubbles. The amount of 5% dextrose solution used in ALHD varied according to the size of the index nodule and was usually between 30 and 50 mL.
Procedure-related pain was graded into four categories: grade 0, radiofrequency power did not have to be turned off because the patient experienced no pain; grade 1, radiofrequency power was turned off once or twice to reduce pain levels; grade 2, radiofrequency power was turned off more than three times; and grade 3, the procedure was terminated before completion because of severe pain [15,16]. Complications and side effects were defined according to the quality improvement guidelines of the Society of Interventional Radiology and a prior multicenter evaluation of complications [9,17].
After RFA, the initial ablation ratio (IAR), a semi-quantitative index that measures the amount of ablation, was calculated to predict the efficacy of the technique. The IAR is the ratio of the ablated nodule tissue volume (Va) to the total nodule volume (Vt) immediately after RFA, as expressed in the formula IAR=(Va/Vt)×100 (%). Since the ultrasound image immediately after RFA is often unclear because of hemorrhage and edema, Va and Vt are indirectly measured. Vt is the same value as the index nodule volume measured before RFA, whereas Va is calculated using the viable volume measured on ultrasound imaging taken 1 month after treatment (Vv1mo), where Va=Vt-Vv1mo. Therefore, the following formula was used in this study: IAR=(Vt-Vv1mo)/Vt×100 (%) [4,5,18].
Follow-up and Outcome Assessment
Follow-up ultrasonography (US) was performed at 1, 6, and 12 months after RFA, and changes in nodule size and volume were evaluated. Volume reduction was calculated as follows: volume reduction ratio (VRR, in %)=[(initial volume-final volume)×100]/initial volume. Therapeutic success was defined as a volume reduction >50% of the initial nodule volume on a follow-up US examination [19]. The therapeutic success rate was defined as the percentage of successfully treated nodules [20].
Statistical Analysis
Statistical analyses were performed using SPSS for Windows version 23.0 (IBM Corp., Armonk, NY, USA). The long-axis diameter and the calculated volumes of the RFA zones are reported as mean±standard deviation. The diameters and calculated volumes of the ablation zones and ablated nodules obtained at each follow-up examination were compared using the Student t-test. All P-values were two-sided, and P<0.05 was considered statistically significant.
Results
Patient Demographics and Clinical Characteristics
The 39 patients with biopsy-proven benign thyroid nodules underwent a total of 41 RFA sessions. Table 1 shows the baseline characteristics of the patients and nodules. The mean longest dimension and volume of the index nodules were 4.2±1.4 cm (range, 1.6 to 8.1 cm) and 20.5±21.6 mL (range, 1.0 to 108.5 mL), respectively. The mean total radiofrequency (RF) energy used was 2,296.8±1,906.1 J (range, 519.7 to 11,168.0 J). The treatment characteristics of the 41 RFA sessions are listed in Table 2. More than 30 mL of 5% dextrose solution was used in each case. In all patients, ALHD adequately controlled pain during the procedure. No patient received an additional lidocaine injection after the initial use of 5–10 mL at the start of the procedure.
Treatment Outcomes in the Clinical Study
The mean IAR was 90.7%±8.3% (range, 70% to 100%). Table 3 shows changes in size and volume over time after treatment. After RFA, significant reductions in the mean volume of the ablated nodules were noted at 6- and 12-month follow-up visits (P<0.001). Among the 39 patients, 24 had achieved therapeutic success at the 6-month follow-up and 37 had achieved therapeutic success at the 12-month follow-up. The therapeutic success rates were 61.5% (24/39) and 94.9% (37/39) at the 6- and 12-month follow-up visits, respectively. After the procedures, both symptom and cosmetic scores showed significant decreases at the 6- and 12-month follow-up visits (P<0.001 for both).
Safety
During RFA of the nodule margin, almost all patients complained of pain, which was controlled by continuous ALHD instead of lidocaine. All patients tolerated the procedure. Transient voice change was observed in one patient, but the patient recovered spontaneously within 30 minutes of cessation of the RFA. At the time when the patient’s voice change was noticed, additional cold (0°C–4°C) 5% dextrose solution was immediately and continuously injected into the tracheoesophageal groove according to the routine management protocol for suspected nerve damage [21]. No patient experienced a complication requiring hospitalization or a delayed complication during follow-up.
Discussion
ALHD was technically feasible in all patients included in this study cohort. ALHD provided good pain control without additional lidocaine injections, and venous staining was therefore effectively achieved from the marginal venous ablation, which made near-complete ablation of the index nodule possible, as reflected by the high IAR (90.7%). As a result of this high IAR, the VRR at 12 months was 76.3%±18.9%, and the therapeutic success rate was 94.9% (37/39). There was no major complication requiring hospitalization or delayed complications related to the RFA procedures.
The major role of ALHD is to minimize marginal regrowth by achieving a high IAR. It is well known that the final VRR is related to the size of the index nodule, and larger index nodules require more ablation sessions to achieve sufficient volume reduction [3,5]. In a previous study by Lim et al. [3], the number of treatment sessions required to achieve sufficient volume reduction was higher in cases with an index nodule volume >20 mL, and all regrowth arose from the undertreated peripheral portion of the nodule. Therefore, the marginal venous ablation technique and complete tumor ablation, which are represented by venous staining signs and a high IAR, respectively, are important to prevent marginal recurrence. Sim et al. suggested that an IAR of more than 70% could be used as an indicator of expected therapeutic success [5]. In this study, although the mean initial nodule volume was large (20.5±21.6 mL), the mean IAR was high enough to expect therapeutic success (90.7%±8.3%) and the therapeutic success rate at 12 months was 94.9%.
The further roles of ALHD are pain control and prevention of thermal damage to critical structures around the thyroid gland. There are no sensory nerves inside the thyroid gland, but they are abundant in the thyroid capsule and strap muscle. In terms of pain control during RFA, lidocaine can control pain from the thyroid capsule and ALHD can control strap muscle pain. The pain induced by the RF shows an inverse relationship with distance. Therefore, injecting fluid to maintain a separation of 5 mm or more between the thyroid margin and strap muscle can control muscle pain. Compared with a previous study of RFA of benign thyroid nodules by the thyroid team of the authors’ affiliated institution [22], the pain scores during RFA tended to be lower using the hydrodissection technique (1.0±0.7 vs. 0.8±0.9). Thermal damage to the perithyroidal structures may be induced when applying the marginal venous ablation technique, especially for thyroid nodules located at the periphery of the thyroid gland. Thus, when the index nodule is located close to important neck structures, including the recurrent laryngeal nerve, common carotid artery, trachea, and esophagus, complete ablation of the index nodule achieving the venous staining sign is difficult. However, in this study, a safety margin was achieved using the ALHD technique during the procedure, overcoming the limitations and difficulties of the marginal ablation of index nodules located near important neck structures. ALHD with a continuous injection of cold 5% dextrose solution could easily cover not only the lateral compartment, but also the posterior compartment.
General anesthesia or sedation for pain control is not generally recommended for RFA due to the risk of delayed detection of complications during the ablation, resulting in more serious complications [14,23]. With local anesthesia during the ablation procedure, the physician can check for signs of complications such as voice change, eye movement, and irritated trachea signs. In contrast, under general anesthesia, several cases of complications including trachea injury, skin burn, and recurrent laryngeal nerve injury have been reported with ablation procedures [24-26]. For pain relief during RFA, local anesthesia obtained through injection of lidocaine at the skin puncture site and into the perithyroidal area is recommended by the Korean Society of Thyroid Radiology [14,27] and is the method mainly used by physicians. Although systemic lidocaine toxicity is a rare complication, it can be life-threatening, with symptoms of circumoral numbness, dizziness, and nausea following hypotension and bradycardia [28,29]. Lidocaine toxicity is strongly correlated with the total dose and rate of absorption, which depend on the blood supply to the tissue [30,31]; therefore, to prevent and minimize systemic toxicity, there is a limit to the total dose of lidocaine that can be given. The experience gained over the course of the procedures described in this study suggests that an injection of cold 5% dextrose solution with the hydrodissection technique, rather than a further injection of lidocaine, can provide effective pain relief when a patient complains of pain. Therefore, the total amounts of lidocaine used during the procedure were relatively small, although the pain was well-controlled. Furthermore, the patients were able to remain in a comfortable state during the procedure.
ALHD has the following advantages compared to other procedures. First, the needle can be placed in the anterior portion and fixed in place, and the hydrodissection technique can be applied with relatively little movement of the needle. Second, the 5% dextrose solutions injected from the anterior aspect can reach the lateral, posterior, and even medial aspects of the thyroid gland as the amount of injected solution increases. Third, ALHD can be applied using the same needle injection site used for lidocaine. A possible limitation of ALHD is inadvertent injection of 5% dextrose solution into strap muscle or thyroid parenchyma. Therefore, experienced interventional skills and anatomical knowledge are necessary to apply ALHD. Four types of hydrodissection have been suggested [12], and of these, the anterolateral approach has several advantages, as described herein. The posterior approach is usual for treating parathyroid adenomas or recurrent tumors close to the danger triangle. The pre-tracheal approach is useful for treating isthmus masses, and the danger triangle approach is useful for treating nodules at the danger triangle.
This study has several limitations. First, the number of cases of RFA performed with ALHD was small, making it difficult to determine whether this technique should be adopted as standard treatment. Large-sized prospective studies are required to determine a standard treatment strategy for the ALHD technique during RFA. Second, the procedures involving ALHD were performed by an experienced radiologist. An operator with less expertise would require learning time to apply ALHD during RFA. Third, although a mean IAR of more than 90% and a VRR of more than 70% were achieved at the 12-month follow-up, longer-term follow-up results are necessary to evaluate the actual clinical effectiveness of ALHD. Fourth, the complications, side effects, and assessment of pain during the procedure were evaluated symptomatically, on the basis of subjective complaints by the patients, not by objective and quantitative criteria. Fifth, because of the retrospective nature of this study, the exact amount of 5% dextrose solution and lidocaine used was unclear. Future studies with exact records of the amount of 5% dextrose solution and lidocaine used are needed.
In conclusion, this study found that the ALHD technique was technically feasible in all patients and effective for achieving near-complete ablation of the index nodule, resulting in a high IAR. The ALHD technique also had a pain-relieving effect, resulting in low quantities of lidocaine administration during the procedure.
 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI



