

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Imaging the fine-meshed network of the lymphatic system has remained a major challenge, as it is difficult to access with various contrast agents, unlike the usual contrast examinations performed in the radiology department. An accurate and sensitive imaging technique is required to visualize the lymph vessels and flow to identify abnormalities such as lymphedema and lymphangiectasia. This is necessary to obtain a correct diagnosis and create a patient-specific therapy plan. Over the years, several imaging techniques have emerged to enable the visualization of the peripheral lymph vessels and their flow, each with its own advantages and limitations.
Lymphangiography of the extremities can be performed by injecting ethiodized oil as a contrast agent, either inter-digitally or directly into a lymph vessel in the foot. In lymphoscintigraphy, a radioactive agent (99mtechnetium nano-colloid) is injected inter-digitally and its path is then followed through the extremities, with the resulting images being low-resolution. Alternatively, the superficial (peripheral) lymphatic vessels can be visualized using indocyanine green; however, this is a time-consuming technique that also results in low-resolution images. Other radiological modalities, such as magnetic resonance imaging, computed tomography, and fluoroscopy [1,2], can be used for lymphangiography after a minimally invasive inguinal intranodal contrast injection, enabling the visualization of the central, para-aortoiliac lymphatic vessels. This can be of diagnostic relevance in cases of chylothorax or chylous ascites [3,4]. These methods are all laborious and time-consuming.
In search of a more easily applicable, high-resolution, and dynamic modality, state-of-the-art ultrasound techniques could be applied to image superficial lymphatic vessels. These techniques have also been able to provide slow-flow information. The use of contrast-enhanced ultrasonography (CEUS) with an intranodal injection of microbubbles (Sonovue, Bracco, Milan, Italy), has proven valuable for imaging both central [5] and peripheral lymphatic vessels [6,7]. Dynamic imaging gives insights into the flow direction, which can be normal antegrade, abnormally retrograde, or both. Furthermore, several ultrasound manufacturers have recently developed microvascular flow imaging (MVFI) techniques (e.g., Superb Microvascular Imaging [SMI] by Canon Medical Systems, Tokyo, Japan; Micro Flow Imaging by Philips Medical Systems, Best, The Netherlands; Slow Flow by Siemens Healthineers, Erlangen, Germany; Microvascular Imaging by GE Healthcare, Chalfont St Giles, UK; and MV-flow by Samsung Healthcare, Seoul, Korea). These techniques use different algorithms from the conventional Doppler techniques, in order to visualize slow-flow velocity and small-diameter (blood) vessel flow. MVFI could play a role in the niche where CEUS is used [8]. Some studies have even suggested that MVFI is a valuable alternative to CEUS [9,10].
Due to the improved resolution of ultrasound machines and their potential to image low-flow velocities, the combination of high-resolution ultrasonography (HR-US) and MVFI could be applied to the imaging of vessels that transport fluids at very slow rates. The authors have started to explore the potential of using HR-US and MVFI in imaging the superficial lymphatic vessels. This technical note presents the first results.
Materials and Methods
Compliance with Ethical Standards
Approval from the local ethics committee (Commissie Mensgebonden Onderzoek–CMO 2020-6651) was obtained for this single-center study. All patients provided written informed consent.
Patients and Study Design
The participants (n=84) who received lymphatic ultrasound examinations were patients with suspected central or peripheral lymphatic disorders (for example, lymphedema, chylothorax/chyluria, traumatic or iatrogenic lymphatic leakages, and/or congenital lymphatic anomalies), who underwent diagnostic contrast-enhanced MR-lymphangiography (DCMRL). The patients were between 0 and 86 years old. There were no exclusion criteria for ultrasonography prior to DCMRL.
Ultrasound Examinations Using the Intranodal Technique
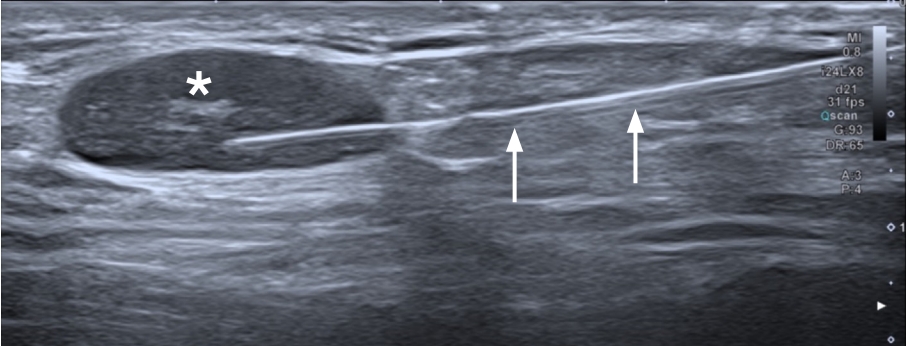
All examinations were performed by a single radiologist with more than 10 years of experience in ultrasonography, between December 2018 and December 2022, with a Canon i800 series using an i24LX8 linear matrix transducer (Canon Medical Systems), equipped with SMI. Both inguinal areas were examined prior to DCMRL, with the patient in the supine position, in order to detect suitable lymph nodes for intranodal injection. HR-US was used while placing the intranodal needle [1]. The needle tip was placed at the corticomedullar border (Fig. 1).
Microvascular Flow Imaging
After the placement of one intranodal 25G needle (Pencan, B. Braun Medical B.V., Oss, The Netherlands) in the inguinal lymph nodes on each side, HR-US was used to visualize the lymphatic flow from these lymph nodes. The monochrome version of MVFI in Canon’s SMI (mSMI)-box was activated with a maximum velocity of 1.0 cm/s in order to visualize the lymphatic flow. A small amount (approximately 2 mL) of saline solution (0.9% NaCl) was injected at a rate of 0.5-1.0 mL/min and visualized using HR-US with mSMI.
The saline solution was used as a contrast agent to visualize the antegrade, efferent flow (i.e., in the cranial direction away from the inguinal lymph node). To qualitatively assess the flow, the saline solution must be injected and cine loops must be created. Ultrasound images and the correlation between HR-US and the results of the DCMRL can be reviewed. In cases of dilated lymph vessels, dilation is visible on grayscale images without the introduction of a saline solution. Vessels are classified as dilated if no flow is detected and the diameter is larger than the usual 1-2 mm in the lower extremities [11]. Flow images should be revised by looking at the direction of the flow and the progression of the saline solution into the surrounding tissues. Flow is classified as antegrade (efferent) when it travels in the cranial direction, with a slow velocity (in accordance with the injection rate) or as retrograde when it travels in the caudal (afferent) direction. The needle position can be considered inadequate if the injected fluid accumulates around the lymph node and seeps into the surrounding dermal tissues (dermal backflow) or if the efflux demonstrates fast (venous) flow, which could also be a sign of lympho-venous shunting.
Exemplary examinations demonstrating pathologic findings are included in the Results section.
Results
Normal Sonographic Findings
Lymph enters the lymph nodes via the convex side, on which the afferent lymphatic vessels are drained. The lymphatic vessels contain valves that allow the lymph to flow solely in the antegrade (cranial) direction. When assessing the lymph nodes and surrounding tissue using mSMI at 1.3 cm/s, no lymphatic flow was measured. The velocity was selected in order to visualize the applied flow, but not limit the effects of artifacts. When moderate pressure was applied with a syringe, antegrade, gently pulsating lymphatic flow was visualized in the efferent lymphatic vessels (Fig. 2, Video clip 1). After releasing the syringe pressure, lymphatic flow gradually stopped and was no longer visible after a few seconds (Video clip 2). The visibility was limited to only the locoregional area of the intranodal-approached lymph node.
Abnormal Sonographic Findings
In cases of lymphedema in the lower extremities, possibly caused by congenital thoracic duct aplasia, iatrogenic and traumatic injuries, or chronic high pressures in the lymphatic system (secondary to high venous pressure), the peripheral lymphatic vessels can become dilated or obstructed. This causes the saline solution to flow in different directions (antegrade and retrograde). The following paragraphs describe these pathologies.
Lymphangiectasia and dermal backflow
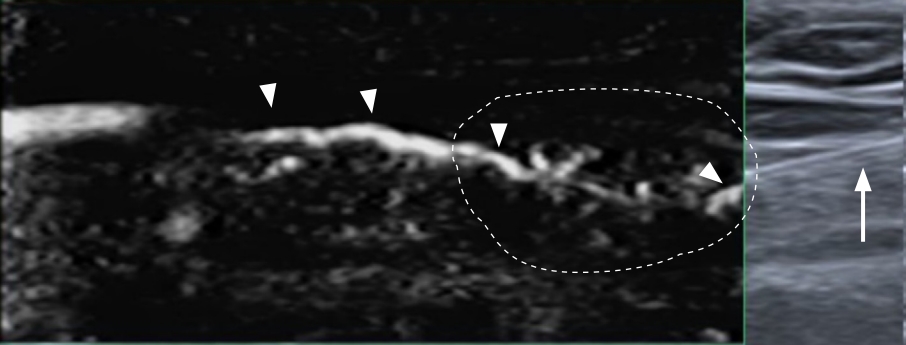
In some cases, dilatation can lead to backflow into the dermal layers, causing lymphedema. When assessing this phenomenon, flow out of the lymph node into the efferent lymphatic vessel is seen and its tortuous trajectory is visible (Fig. 3). After injecting additional saline solution, the backflow becomes evident when the saline seeping into the ventral dermal layers.
Lymphangiectasia and retrograde lymphatic flow
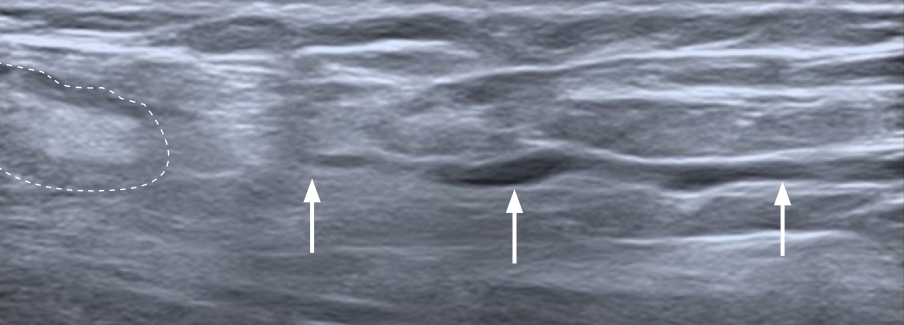
Dilated peripheral lymphatic vessels can be visualized using B-mode ultrasonography (Fig. 4). When applying only minimal pressure with the ultrasound probe, the vessels are discernable as tubular structures without any conventional Doppler flow. Dilation can cause the lymphatic valves to become insufficient, leading to lymphatic stasis.
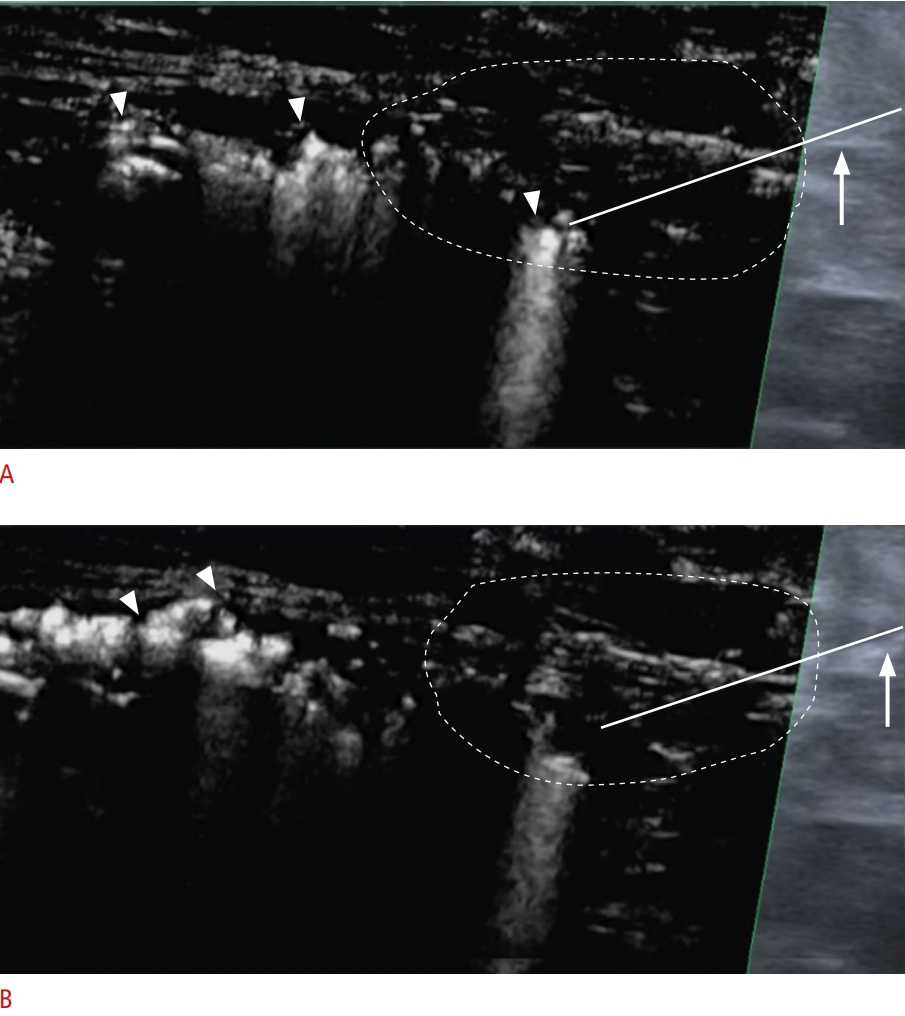
In case of leaking lymphatic valves, the injection of a saline solution can lead to retrograde flow in the peripheral lymphatic vessels (Fig. 5). After injecting saline solution, flow is seen in both antegrade and retrograde directions (Video clip 3). Flow rates are difficult to quantify due to the too-low frame rate in this application in the triplex mode, in which grayscale, SMI, and pulsed-wave Doppler are visible. A qualitative assessment shows that the saline solution flows in a retrograde direction.
Extravasation
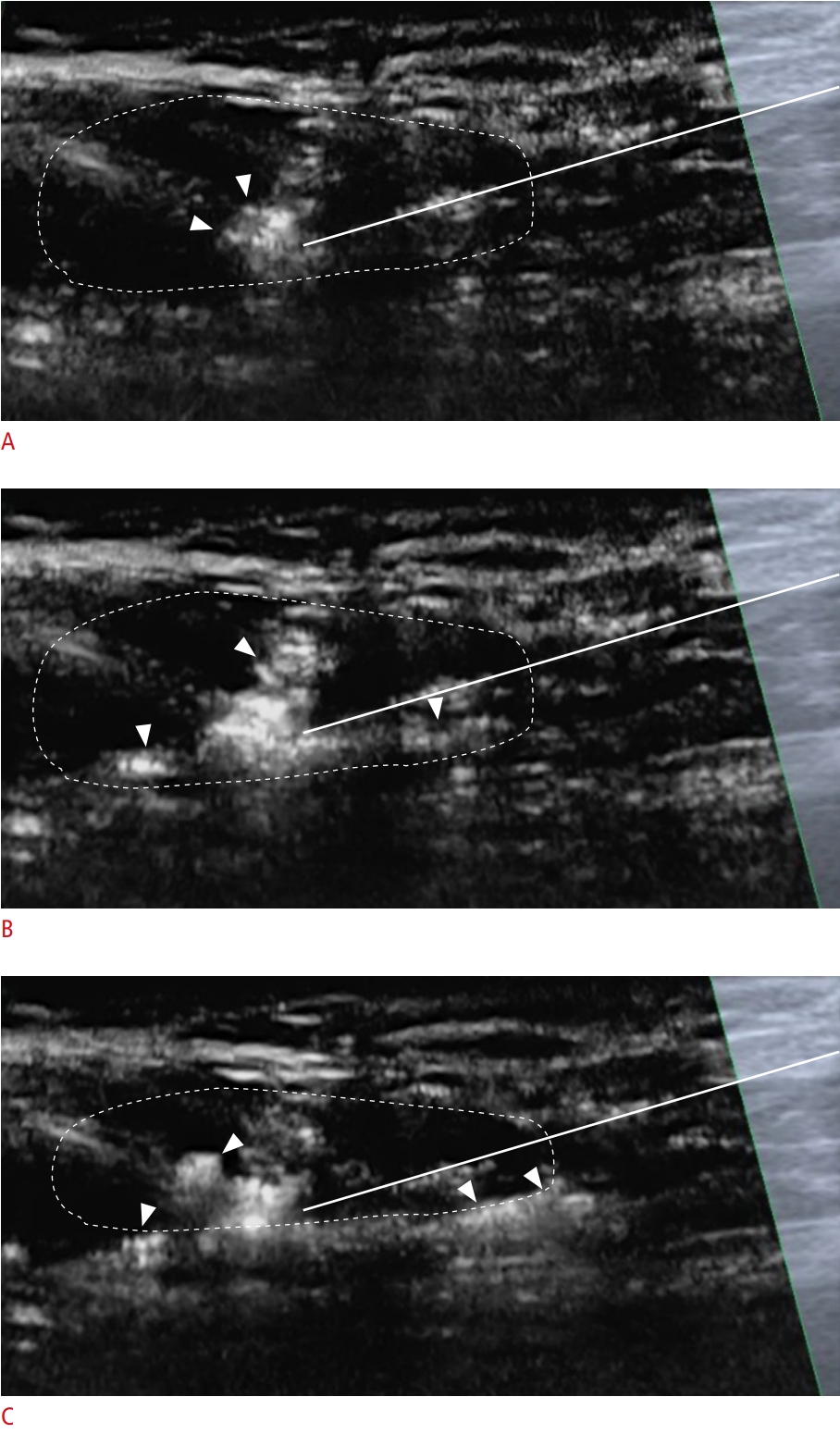
In case of incorrect needle placement or luxation of the needle, extravasation of the fluid can occur (Fig. 6, Video clip 4). As the contrast agent used is 0.9% NaCl saline solution, this is harmless to the patient, although it can be painful. If no lymph node is located, the procedure should be repeated in order to find the correct needle placement to visualize the lymphatic vessels.
Discussion
The main finding of this study is that HR-US seems to be a valuable method for visualizing the superficial lymphatic vessels and flow. It was possible to distinguish normal antegrade from abnormal and retrograde flow, as well as normal from ectatic lymph vessels.
Until recently, conventional B-mode ultrasound techniques were not suitable for imaging small lymphatic vessels or measuring very slow lymphatic flow. However, recent technical advances have made ultrasonography a potential lymphatic imaging modality due to major improvements in temporal and spatial resolution, leading to the development of HR-US. Previously, HR-US using transmitted frequencies above 15 MHz, was only feasible using specialized, pre-clinical imaging systems [12]. Recent developments in transducer technology have produced a clinical transducer operating up to 29 MHz, resulting in HR-US images with an extremely high resolution of 70 μm [13]. Conventional color Doppler flow imaging (CDFI) uses a filter to remove motion, clutter, and wall artifacts, but low-flow information is removed as well. The algorithm of MVFI analyzes clutter not only in the temporal domain, but also in the spatial domain. This results in improved removal of the wall and motion artifacts, while preserving low-flow information. Consequently, MVFI provides images with very slow flow, down to 0.3 cm/s (0.3 cm/s is the lowest velocity that can be utilized on the scale of SMI. No documentation regarding minimal flow velocity is available at this moment).
Imaging of the lymphatic vessels has always been a challenge [4], and each imaging method has its disadvantages, such as being laborious or having low temporal or spatial resolution. In search for a more easily applicable imaging modality, HR-US with MVFI has potential as a relatively inexpensive, dynamic, and fairly quick technique to image superficial lymphatic vessels. MVFI has the advantage of high frame rates, high sensitivity, and—due to its algorithm—a reduced presence of artifacts, potentially making it a feasible technique for detecting slow superficial lymphatic flow [14,15]. The mSMI mode improves flow sensitivity by subtracting the background information from grayscale images and focusing only on the flow in the vessels [8]. SMI has been studied for use in the detection of sentinel lymph nodes and micro-vascularization in superficial tissues and organs, providing additional information in ultrasound examinations [9,14]. The advantage of SMI over CDFI is that with SMI, most of the hindering motion artifacts are removed, thus revealing the true flow [15,16]. The patency of thoracic duct outflow has been studied using CEUS [17]. Previous studies have investigated the applicability of MVFI in characterizing thyroid lesions [16,18,19] and renal masses [10] in comparison to CEUS. Some studies have compared the efficacy of both CEUS and MVFI for various applications [10], suggesting that MVFI is a valuable alternative for CEUS [9,10] or may even function as a replacement for CEUS in certain cases [8,18]. With the intranodal technique, imaging is limited to only the locoregional area of interest, due to the fact that the lymphatic flow is visualized using the pressure applied using the syringe. Malposition of the intranodal needle can lead to venous outflow after the injection of saline. This may be seen as diluted and relatively fast outflow. The venous vessels are larger than the lymph vessels and will possibly show a lower intensity in the mSMI-box due to the dilution of the flow within the slow bloodstream. Lympho-venous shunting is expected to show similar venous flow, but this possibility requires further investigation.
Smooth muscle cells in the lymphatic wall, adjacent muscle contractions, arterial flow, and respiratory movements of the chest cavity all contribute to antegrade lymphatic flow [11]. This study found that in cases of high systemic (iatrogenic or traumatic) lymphatic pressure, lymphedema, or abnormal anatomy, MVFI can be used to determine retrograde flow or local flow into the dermal layers. In line with previous studies that assessed other body parts, HR-US and MVFI were found to be useful additional tools for imaging superficial lymphatic vessels. Further investigations could determine whether HR-US and MVFI are feasible in diagnostic examinations of superficial lymphatic abnormalities.

 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI



