

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Ductal carcinoma in situ (DCIS) is defined as a malignant proliferation of epithelial cells confined to endothelial lobular units without invading the basement membrane [1]. The prevalence of DCIS has increased with the widespread practice of breast screening through mammography. In the United States, the prevalence of DCIS was 1.87 per 100,000 in the 1970s before mammography screening programs, accounting for less than 5% of all breast cancers. However, the prevalence increased to 32.5 per 100,000 in 2004 [2-5]. Although DCIS accounts for more than 20% of breast cancers diagnosed in the United States, the assumption that all cases of DCIS are precursor lesions of invasive breast cancer has been questioned in recent years [6-8].
The most common finding of DCIS is the presence of microcalcifications in the mammography screening of asymptomatic patients [2,9]. Breast ultrasonography is considered to be an adjunct to screening mammography, although breast ultrasonography is superior to mammography in detecting lesions in patients with symptomatic DCIS [10]. The most common ultrasonographic findings of DCIS are a hypoechoic mass with an irregular shape and indistinct margin [11,12]. Additional findings include microcalcifications, ductal changes, or structural distortions [11-18].
Even though it is impossible to predict with certainty whether DCIS will progress to invasive disease, histologic features classified according to the microscopic findings of DCIS provide important information on its prognosis. It has been reported that a high nuclear grade, a solid or cribriform architectural pattern, and comedonecrosis are associated with a high recurrence rate when conservative treatment is performed [5,19,20]. Biological markers can also provide information useful for predicting the biological response, pathologic progression, treatment response, and tumor recurrence in patients with DCIS [21,22]. The estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2), and the Ki-67 index are the most studied biological markers. They have been routinely measured to predict the risk associated with DCIS [21,23,24]. When DCIS develops into invasive breast cancer, ER and HER2 status and the breast cancer subtype are usually maintained [6,25].
To date, some studies have presented the ultrasonographic features of pure DCIS, but few studies have reported comparisons between the ultrasonographic findings and pathologic features of pure DCIS [10,12,14,15,17,23,26]. The evaluation of ultrasonographic features in correlation with the pathologic and biological features of DCIS will provide valuable clues to predict the prognosis of the disease, and the purpose of this study was therefore to evaluate the ultrasonographic features of pure DCIS and to investigate the correlations of ultrasonographic features with pathologic and biological features.
Materials and Methods
Patients
This retrospective study was approved by the Institutional Review Board of our institution for patients' record and consent to use of information. From December 2003 to April 2016, 178 patients were diagnosed with pure DCIS based on pathologic findings. Thirty-two patients who did not undergo ultrasonography before excisional biopsy and five patients who had no history of surgical biopsy were excluded from this study, as well as three patients without mammograms were also excluded. Of the remaining 138 patients who were diagnosed with pure DCIS, 3 had bilateral lesions. Ultimately, 141 ultrasonographic findings in 138 women (mean, 51.3 years; range, 28 to 83 years) were included in our study for the evaluation of the imaging features of pure DCIS (Fig. 1) and the investigation of correlations with pathologic features and prognostic biomarkers (Fig. 1). Sixty-four patients (46%) were symptomatic. Of the symptomatic cases, 47 had palpable masses, 12 had discharge, three had pain, and two had nipple eczema.
Ultrasonographic Analysis
Ultrasonography was performed by a breast radiologist using a broad-band 5-12 MHz linear array transducer (LOGIQ E9, GE, Wauwatosa, WI, USA) or a broad-band 5-17 MHz linear array transducer (iU 22, Philips, Seattle, WA, USA). Ultrasonography was performed on both breasts according to our hospital's basic screening method. Two orthogonal images and color Doppler images were obtained on the axial and vertical planes when the lesion was seen. Additional images were obtained based on the radiologist's decision. The ultrasonographic findings were analyzed by consensus by breast imaging specialists who had 14 years of experience in breast imaging, along with one resident who had been trained for more than 5 months, using a picture archiving and communication system monitor. Lesions were analyzed using the terms of the American College of Radiology Breast Imaging Reporting and Data System (BI-RADS) lexicon [27]. In addition, to describe lesions that were difficult to define as mass lesions on the ultrasonographic findings of DCIS, the lesion pattern was classified as a mass lesion, non-mass lesion, or ultrasonographic occult lesion based on the guidelines of the Japan Society of Ultrasonics in Medicine [28]. Mass lesions were defined as lesions for which the mass was different from the surrounding tissue and constituents. Non-mass lesions were defined as lesions that were difficult to diagnose as a mass. The size, shape, margin, echo pattern, orientation, and color Doppler images of mass lesions were analyzed. Echogenic foci suspected of microcalcifications on ultrasonography were considered positive only when corresponding microcalcifications were seen on mammography. Ultrasonographic ductal changes were considered to be present when there was a cystic dilatation of an irregular duct branching from malignant lesions, intraductal masses, or debris. The presence of architectural distortion accompanying the lesion was also analyzed.
Histopathologic Analysis
Pathologic specimens were analyzed by a pathologist with more than 10 years of experience. The nuclear grade was classified as low, intermediate, or high based on the Van Nuys classification. The presence of comedonecrosis was also analyzed. Immunohistochemical analysis was performed for ER, PR, HER2, and the Ki-67 index. ER and PR positivity was defined as nuclear staining of at least 1% positive tumor nuclei [29]. HER2 was scored as 0 (no staining), 1+ (weak and incomplete membrane staining), 2+ (strong, complete membrane staining in ≤30% of tumor cells or weak/moderate heterogeneous complete staining in ≥10%), or 3+ (strong, complete membrane staining in >30% of tumor cells) through an immunohistochemical analysis [30]. We performed silver-enhanced in situ hybridization (ISH) for all equivocal cases (2+ immunohistochemical staining) using the Inform HER2 Dual ISH DNA probe cocktail (Ventana Medical Systems Inc., Tucson, AZ, USA) to evaluate HER2 expression using a standard method. The Ki-67 index was determined as the percentage of tumor cells that exhibited nuclear staining. The Ki-67 index was divided into low-grade (<5%), intermediate-grade (6%-19%), and high-grade (≥20%) based on the rate of positive nuclear staining of cancer cells, following previously established guidelines [31,32].
Statistical Analysis
Statistical analysis was performed by dividing the lesions into mass lesions and non-mass lesions. The frequency of various factors according to the lesion type was evaluated. Ultrasonographic findings were compared with pathologic findings (nuclear grade and presence of comedonecrosis) and biological factors according to the presence of microcalcifications and ductal changes. As the comparative analysis variables showed a normal distribution, a parametric analysis method (the chi-square test) was used. P-values <0.05 were considered to indicate statistical significance. Statistical analysis was performed using SPSS software ver. 20.0 (IBM Corp., Armonk, NY, USA).
Results
Ultrasonographic Features of Pure DCIS
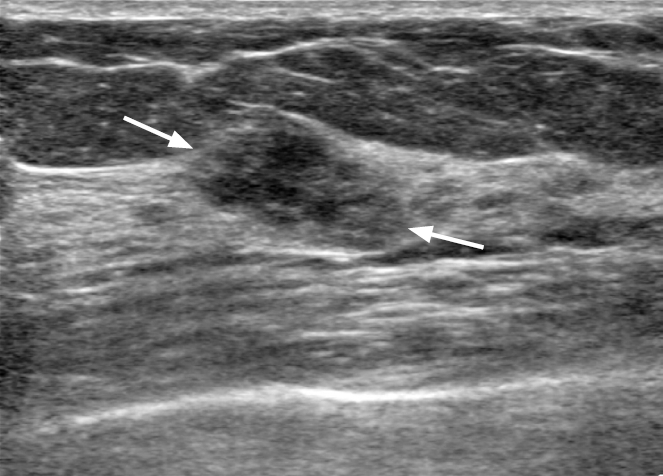
Regarding ultrasonographic findings, mass lesions were found in 75 cases (53.2%) (Fig. 2), non-mass lesions in 56 cases (39.7%) (Fig. 3), and ultrasonographic occult lesions in 10 cases (7.1%). The most common shape of pure DCIS was irregular (46 cases, 32.6%). In addition, 18 cases (12.8%) were oval and 11 (7.8%) were round. Fifty-seven cases (40.4%) showed a non-circumscribed margin, while only 18 (12.8%) showed a circumscribed margin and 39 (27.7%) had an indistinct margin. Hypoechogenicity was the most common echo pattern (53 cases, 37.6%). The orientation of the mass was non-parallel in 50 cases (35.5%) and parallel in 25 (17.7%). The average size of the mass lesions was 1.3 cm (range, 0.4 to 2.7 cm), and that of the non-mass lesions was 2.0 cm (range, 1.2 to 5.3 cm). Forty-eight cases (36.6%) showed microcalcifications and 21 (16.0%) showed ductal changes, which were more frequently observed in non-mass lesions (Fig. 4). Six cases (4.6%) of non-mass lesions with architectural distortion were also found. Color Doppler examination data were available for 108 cases, including 60 (55.6%) without increased blood flow and 48 (44.4%) with increased vascularity (Table 1).
Comparison with Pathologic and Biological Features
When the ultrasonographic and pathologic findings were analyzed, non-mass lesions on ultrasonography were significantly correlated with a high nuclear grade (P=0.004) and comedonecrosis (P=0.006) in comparison to mass lesions. The ultrasonographic finding of microcalcifications was also significantly associated with high nuclear grade and comedonecrosis (P<0.001 for both) (Table 2).
When correlations between the characteristic findings of ultrasonography and biological markers were analyzed, the ultrasonographic presence of microcalcifications showed a statistically significant association with a Ki-67 index higher than 20% (P<0.001) and HER2 positivity (P=0.003) (Table 3).
Discussion
The ultrasonographic findings of pure DCIS have been presented in several studies, and the findings of our study are similar to those of previous reports [10-12,14-18,26]. In our study, the most common ultrasonographic appearance of DCIS was a mass lesion. Approximately 53.2% of cases were irregular and hypoechoic masses without a circumscribed margin. Although these findings of DCIS were indistinguishable from those of invasive ductal carcinoma, our results are consistent with those of previous studies showing that the most common ultrasonographic finding of DCIS was a mass in approximately 52%-88% of cases [10-12,14-18,26]. Scoggins et al. [10] reported that a visible lesion on ultrasonography was present in 52% of 691 patients with pure DCIS and that 76% of those cases had mass lesions. Park et al. [12] analyzed 76 cases of pure DCIS (48 asymptomatic and 25 symptomatic), and found that 75% of the lesions were visible on ultrasonography. A morphologic analysis found that 50% of non-high-grade DCIS cases showed an irregular shape with an indistinct and microlobulated boundary and a hypoechoic mass. In our study, a lesion visible on ultrasonography was present in 92.9% of cases (131 of 141), which is higher than prior studies. The reason for the higher rate of lesion detection on ultrasonography in our study may have been related to the fact that 45.4% of the patients were symptomatic, in contrast to previous studies. In addition, this tendency might also be related to the fact that patients who had microcalcifications on mammography and underwent an excisional biopsy without ultrasonography may not have been included in our study.
In the present study, although the most common ultrasonographic finding of pure DCIS was a mass lesion, microcalcifications and ductal changes seen on ultrasonography were more common in non-mass lesions than in mass lesions. Ultrasonographic ductal abnormalities or dilatation is not a common finding in DCIS, and have been reported to be present in 4.6%-5% of cases [12,15]. In contrast, in our study, 16% of patients had ductal changes, which is a higher rate than has previously been reported. It has been suggested that dilatation of the duct might be due to necrosis in tumor cells, necrosis in the lumen of the duct, or a lymph-forming reaction around the duct [11].
In our study, microcalcifications on ultrasonography showed a significant correlation with a high nuclear grade and comedonecrosis. In previous studies of the radiologic and pathologic findings of pure DCIS, microcalcifications on mammography and ultrasonography have been reported to be associated with poor pathologic prognostic factors, such as a high nuclear grade or comedonecrosis [10,16,33]. In the ultrasonographic findings of pure DCIS, microcalcifications have been reported to be more common in high-nuclear-grade lesions than in low-nuclear-grade lesions [12]. They have also been more frequently reported in cases with comedonecrosis than in cases without comedonecrosis [10].
Biological markers such as ER, PR, HER2, and the Ki-67 index in pure DCIS cases were also analyzed in our study. Unlike previous studies, our study compared the ultrasonographic findings of pure DCIS with immunologic findings that could predict the prognosis of the lesion. Microcalcifications found on ultrasonography showed a statistically significant correlation with HER2 positivity or an increased Ki-67 index. These results suggest that the ultrasonographic imaging of DCIS may provide meaningful information for predicting its prognosis based on pathologic findings and some biological markers. Previous studies have reported that frequent local recurrence of DCIS was associated with ER negativity, PR negativity, HER2 positivity, and an elevated Ki-67 index [23]. It has been suggested that HER2 and the Ki-67 index might be significant prognostic factors for predicting recurrence after conservative surgery for DCIS [34]. Yao et al. [35] reported that a high Ki-67 index with HER2 positivity in DCIS in the presence of microinvasion was correlated with microcalcifications seen on ultrasonography.
This study has several limitations. First, the number of patients included for screening and the number of patients with symptoms were similar. Additionally, selection bias may have been present because patients with unavailable ultrasonographic findings before biopsy were excluded. Third, the static ultrasonographic findings of pure DCIS were analyzed retrospectively. In addition, although ultrasonographic findings were analyzed jointly with pathologic and molecular biological markers of pure DCIS, mammography findings were not analyzed. Finally, ultrasonography is not a standard technique for evaluating microcalcifications. Therefore, the detection rate of microcalcifications may have been lower than the detection rate that is possible using mammography. Further studies are needed to determine the correlation of microcalcifications between ultrasonography and mammography.
In conclusion, the most common finding of pure DCIS was a mass with an irregularly shaped, indistinct margin and hypoechogenicity. Ultrasonographic microcalcifications and ductal changes were associated with non-mass lesions, which were correlated with poor prognostic factors such as a high nuclear grade, comedonecrosis, HER2 positivity, and an increased Ki-67 index. Ultrasonographic non-mass lesions with microcalcifications require careful management.


 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



