

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Peripheral neuropathies are among the most common neurological disorders [1]. Nerve conduction studies, the current gold standard for detecting and monitoring peripheral nerve disorders, provide objective insights into the functioning of large Aβ nerve fibers [2]. However, they have several limitations. For instance, they are less sensitive at detecting pathological changes in small sensory Aδ or C nerve fibers [3], and they are typically limited to distal nerves, which are often severely damaged and unexcitable in length-dependent neuropathies [4]. A multimodal testing protocol, together with subjective patient-reported outcome measures, has therefore been suggested as the optimal peripheral nerve assessment strategy for several peripheral nerve disorders [5]. In this context, non-invasive imaging techniques, such as nerve high-resolution ultrasonography and ultrasound shear wave elastography (SWE), are emerging adjunct assessment modalities to both electrophysiological and clinical evaluations [6,7].
High-resolution ultrasonography is a rapidly evolving field, offering valuable clinical insights not only into nerve size and morphology [8], longitudinal excursion [9,10] and echogenicity [11] but also into the localization of nerve damage and associated pathological processes [12,13]. However, B-mode ultrasonography does not have the sensitivity required to detect all forms of peripheral nerve disorders and fails to provide information about nerve mechanical properties such as stiffness [7]. Indeed, abnormalities in nerve mechanical properties have been proposed as potential biomarkers for various peripheral nerve disorders [14,15]. For example, animal models of both focal neuropathies and polyneuropathies, including small and large nerve fiber neuropathies, have shown greater peripheral nerve stiffness regardless of the etiology [16-18]. Notably, SWE provides quantitative, real-time, and high spatial resolution elasticity mapping of biological soft tissues by measuring the propagation velocity of shear waves generated remotely using focused ultrasonic beams [19,20]. In peripheral nerves, the shear wave velocity has been shown to be highly sensitive to actual elasticity changes [21], making SWE a promising non-invasive method for evaluating changes in peripheral nerve mechanical properties associated with altered tissue structure and composition [6].
The diagnostic utility of ultrasound SWE has recently been demonstrated. For example, preliminary studies in individuals with carpal [22,23] and ulnar [24] tunnel syndromes, and distal symmetric diabetic polyneuropathy [25,26] have shown an increase in nerve shear wave velocity with the progression and severity of the neuropathy. Studies using ultrasound SWE in lower limb nerves have considerably increased in recent years, either to evaluate clinical conditions such as lumbar radicular pain [27,28] and diabetic polyneuropathy [29,30], or to elucidate nerve biomechanics in healthy individuals [31,32]. Despite its recent popularity and reported validity, variables such as limb positioning, transducer orientation, or the region where the nerve elasticity is assessed, have been suggested to significantly influence the shear wave velocity measures of peripheral nerves [6]. However, it is not fully understood how these, and potentially other, variables may indeed affect the shear wave velocity of the most examined peripheral nerves: the sciatic and tibial nerves. A deeper understanding and mapping of the factors that may influence shear wave propagation within peripheral nerves would be essential for establishing and standardizing SWE assessment protocols, which can be useful for an early diagnosis and the reliable monitoring of nerve-related disorders. The objectives of this systematic review were to summarize the normative shear wave velocity values for the sciatic and tibial nerves in healthy individuals, and to describe the factors that may influence such measurements.
Materials and Methods
An electronic search for experimental or observational studies, written in any language (with at least an English title and abstract), was conducted on PubMed, Embase, and Web of Science. Due to resource constraints for translating articles in non-English languages and a commitment to ensuring accurate analysis, non-English studies were not included in this research. The following keywords, and respective combinations, were used during the search: peripheral nerve, sciatic or tibial nerve, SWE, nerve stiffness, and shear wave velocity. The electronic search was further complemented by reviewing the references of previous reviews and of the included studies. To be included, studies had to use ultrasound SWE to assess the shear wave velocity or shear modulus or Young’s modulus of the sciatic and/or tibial nerves in healthy individuals of any age or sex. Studies in clinical populations reporting shear wave velocity values for healthy controls were also included. The exclusion criteria were as follows: reviews, studies in animals, studies in human cadavers, and studies in clinical populations without healthy control groups.
After selecting the studies, the following data were extracted and summarized in Table 1 [25,26,29,30,32-44]: demographic information of the participants, ultrasound scanner manufacturer, participant’s posture during ultrasound scans, scanned nerve region, transducer orientation used for nerve scans, reliability outcomes, and the shear wave velocity values. To facilitate comparisons, peripheral nerve stiffness values reported in shear modulus (kPa) were transformed into shear wave velocity (m/s), using the following equation: µ=ρVS2, where ρ represents the density of soft tissues (approximately 1000 kg/m3), and VS represent shear wave speed [20]. Soft tissue density is generally modelled as a constant in ultrasound machines, which simplifies the conversion of shear modulus to shear wave velocity. The risk of bias was assessed independently by two authors using the Joanna Briggs Institute Critical Appraisal Checklist for Analytical Cross-Sectional Studies [45].
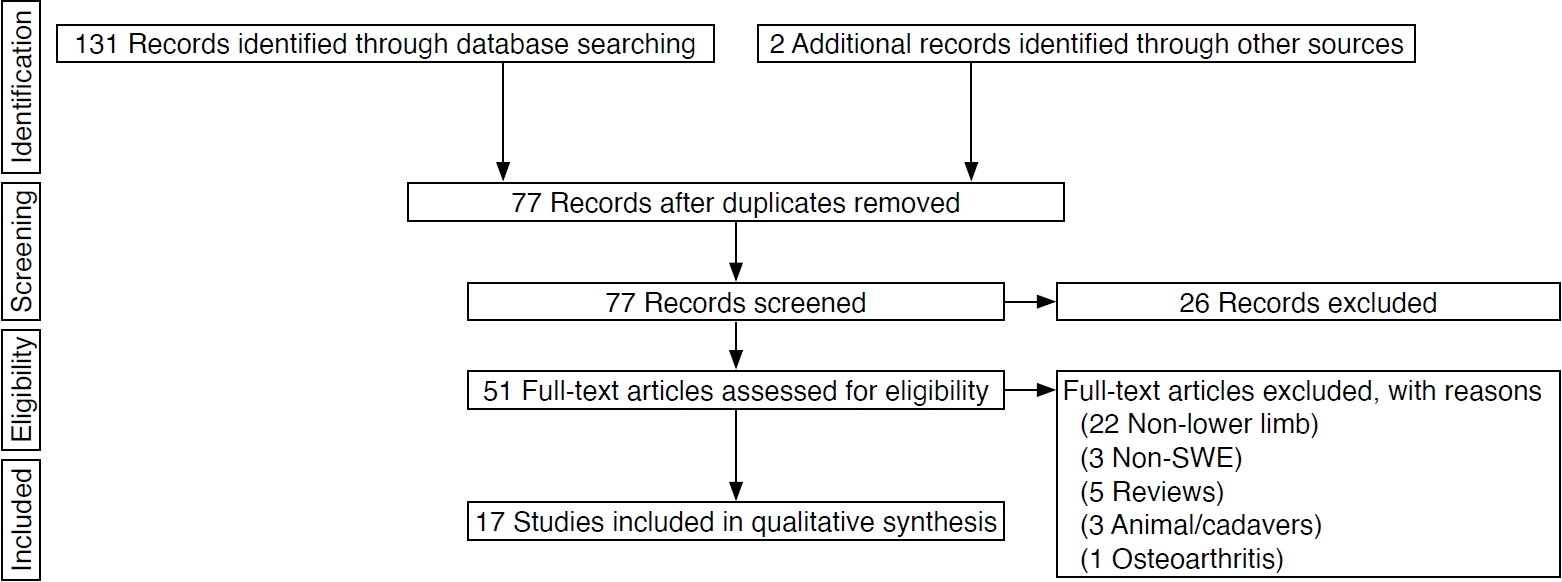
The search strategy and its results are summarized in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram [46] (Fig. 1). The protocol of this review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) with the number CRD42022302947.
Results
Characteristics of the Studies
Seventeen studies were included in the review and are summarized in Table 1. The tibial nerve was assessed in 12 studies, while the sciatic nerve was measured in four studies; one study assessed both nerves.
Tibial nerve shear wave velocity measurements were predominantly conducted with participants in a supine position, with the knee fully extended and ankle in plantarflexion (resting angle); however, an alternative prone position was utilized in three other studies.
For the sciatic nerve, all studies employed a prone position for participants, characterized by full knee extension and a resting ankle angle during shear wave velocity scans.
In most studies, the tibial nerve was assessed above the medial malleolus. In two studies [36,44], the tibial nerve was assessed in the popliteal fossa, and in another study [34], it was measured in three different locations from the popliteal fossa down to the medial malleolus. For the sciatic nerve, three studies [32,33,41] measured nerve shear wave velocity in the subgluteal region, one study measured it in the mid-thigh region [39], and another study [34] measured the sciatic shear wave velocity in two different regions: proximal (i.e., subgluteal) and distal (i.e., proximal to the bifurcation of common sciatic into tibial and fibular nerves).
Risk of Bias Assessment
The included studies showed an overall low risk of bias as the majority of the eight items of the Joanna Briggs Institute appraisal checklist for analytical cross-sectional studies were met. For the studies using a single group of healthy individuals, only items #3 and #4 were not met (i.e., without "exposure" or "condition" to be assessed).
Reliability of the Shear Wave Velocity Measurements
Thirteen studies reported reliability scores for nerve SWE assessments (Table 1). Overall, the use of SWE to measure sciatic and tibial shear wave velocity showed very good reliability, with intraclass correlation coefficient (ICC [2,1]) values ranging from 0.70 to 0.99. The exception is the study of Greening and Dilley [37], which reported only moderate values of reliability (ICC=0.37-0.53). However, the authors suggested that these values may be attributed to methodological disparities, such as variations in the scanner used and the sequence of limb positioning, when compared to other studies of a similar nature.
Shear Wave Velocity of the Sciatic and Tibial Nerves
Table 1 shows the results for nerve shear wave velocities. The reported values show high variability for both the tibial (range, 2.3 to 9.1 m/s) and the sciatic nerves (range, 1.9 to 9.9 m/s). Most of the studies included young adults, while three studies [39,42] compared nerve shear wave velocity between younger and older participants. Hirata et al. [39] showed significantly lower sciatic nerve shear wave velocities in older adults than in younger adults. As for the tibial nerve, conflicting results were observed, with one study reporting higher tibial nerve shear wave velocities in older participants than younger participants [42], while another study [37] found a significant, moderate, and negative correlation (r=-0.58) between the tibial nerve shear wave velocity and age.
Posture-induced changes in nerve shear wave velocity were also investigated by using different lower limb postures through various combinations of hip, knee, and/or ankle angles. For example, one study [34] observed significantly higher sciatic and tibial nerve shear wave velocities (i.e., +54%) with hip flexion, compared to a hip-neutral position. Postures involving full knee extension also resulted in significantly higher nerve shear wave velocities, compared to having the knee flexed at 90°, for both the sciatic [32] and tibial [37] nerves. Similar findings were reported for the influence of the ankle position in the shear wave velocities of the sciatic nerve, with higher shear wave velocities observed with the ankle positioned at higher dorsiflexion angles compared to ankle plantarflexion [33,35,39-41].
Two studies [25,36] assessed the effect of transducer orientation in the shear wave velocity measures. Aslan et al. [25] reported significantly higher shear wave velocities (i.e., with a difference up to 1.8 m/s) obtained with longitudinal transducer orientation (parallel to the nerve fibers) compared to transverse orientation. One study investigated the spatial variation of shear wave velocity along sciatic and tibial nerves [34]. It was observed that distal nerve regions tend to show greater shear wave velocities. For example, an average difference of 1.41 m/s between proximal and distal sciatic has been reported. No studies reported significant left versus right limb differences in sciatic or tibial nerve shear wave velocities.
Discussion
In recent years, there has been a growing interest in the application of SWE to assess peripheral nerve mechanics in both clinical [6] and biomechanical [47] contexts. Shear wave velocity is not only a surrogate measure of nerve stiffness [21], but also a good indicator of tensile loading (i.e., nerve axial stretching) [32] and a promising biomarker for peripheral nerve disorders [6]. The popularity of SWE, especially in contexts of peripheral nerve evaluation, can be further attributed to its non-invasive and painless nature, and its capacity to estimate the mechanical properties of nerves in real time [20,48]. The observed high reliability, as evidenced by the ICC values reported in most of the studies, particularly in the context of intra-examiner measurements, highlights the clinical applicability of SWE. Nonetheless, the findings also point to substantial variability in the normal shear wave velocity values for both sciatic and tibial nerves across studies, which can be attributed to several confounding variables that will be discussed hereunder.
Spatial Variations in Nerve Shear Wave Velocity
The findings of this study indicate that both the sciatic and tibial nerves were assessed at multiple and non-standardized nerve regions across studies. This makes comparisons between studies difficult and may partly explain the large variability in shear wave velocities that has been observed for both peripheral nerves across studies. We identified only five studies [26,29,30,38,43] where a similar assessment protocol was employed, including the same scanner and limb positioning to measure the tibial nerve shear wave velocity in the longitudinal view. The shear wave velocity ranged from 3.9 m/s to 5.7 m/s (mean difference of 1.8 m/s), providing a more realistic notion of the expected variability when using SWE to assess peripheral nerves’ stiffness. Importantly, these normal values for healthy tibial nerves are still considerably lower than the cutoff value of 51.05 kPa (approximately 7.1 m/s) for diagnosing diabetic neuropathy with high sensitivity and specificity [29].
More recently, Andrade et al. [34] found spatial-dependent differences in shear wave velocities in the sciatic and tibial nerves. For instance, shear wave velocity tends to increase in a proximal to distal pattern at both upper and lower leg segments, being greatest in locations near the knee and ankle joints. These observations could be due to regional variations in sciatic and tibial nerves’ ultrastructure, such as thinner and more numerous nerve fascicles wrapped by a thicker perineurium near joints [49], and an increased stiff epineural tissue content in joint regions [50]. Proximity to joint regions has also been associated with distinct nerve material properties in animal models [51]. Moreover, no significant correlations have been reported between nerve shear wave velocity and nerve thickness for both sciatic and tibial nerves [34], suggesting that it is still unclear to what extent nerve geometry influences shear wave velocity measures. However, it should be noted that for thin and stiff tissues such as tendons, the propagation of the shear waves can be guided [52]. Specifically, the shear waves can experience successive reflections on the nerve boundaries, and this phenomenon has the potential to affect the relationship between shear modulus and shear wave velocity [52]. This phenomenon cannot be totally excluded when assessing relatively thin peripheral nerves, and it can bias the quantification of nerve shear wave velocity, especially in neurological disorders known to significantly alter nerve cross-sectional area.
Influence of Limb Posture on Nerve Shear Wave Velocity
Limb posture is an important factor to consider when evaluating nerve shear wave velocity, as it can directly influence the nerve length and, thus, the tensile loading (i.e., the amount of axial stretching). Shear wave velocity is a good indicator of passive forces acting on biological soft tissues, such as muscles [53] and nerves [21]. The findings show that combining knee full extension with hip flexion [34,37] and knee full extension with ankle dorsiflexion [32,39,41] results in a considerable increase in sciatic and tibial nerve shear wave velocity. These observations are consistent with human cadaveric studies reporting an increase in nerve strain in similar lower limb postures [54]. They can be explained by the elastic nature of peripheral nerves, including their inherent layers of connective tissue, when subjected to tensile loads [14]. The elongation of peripheral nerves also results in increased endoneural pressure, which can further contribute to increased nerve stiffness [55]. To minimize variability in shear wave velocity measurements associated with nerve tensile loading during clinical evaluations, it is advisable to opt for scanning postures that mechanically unload the sciatic and tibial nerves, such as maintaining a neutral hip position, flexing the knee, and keeping a resting plantar flexion angle. This would make it possible to isolate true changes in nerve stiffness from potential nerve tensioning caused by postures that subject nerves to stretching, thereby increasing nerve wave propagation velocity.
Mechanical Anisotropy
Assessing peripheral nerves using SWE can be challenging due to their complex structural, mechanical, and geometric characteristics. Peripheral nerves, like other soft tissues in the body, are characterized by their heterogeneous and anisotropic nature, displaying non-linear and viscoelastic properties that lead to stiffening under substantial strains and exhibiting stress relaxation behaviour when axially stretched [14]. In addition to the elastic, heterogeneous, and thin characteristics discussed in earlier paragraphs, it is important to highlight that peripheral nerves exhibit a complex structural organization, which leads to strong anisotropic mechanics. Indeed, the effect of transducer orientation (i.e., along or across the nerve fibers) on shear wave velocity has been well described in anisotropic tissues [56], including peripheral nerves [21]. Measurements of the tibial nerve [25,36] performed with the transducer aligned parallel to the nerve fibers (i.e., longitudinal view) yielded considerably higher shear wave velocities compared to those performed perpendicular to the main direction of the nerve fibers (i.e., transverse scans) [25]. This expected mechanical anisotropy effect should be taken into consideration as a significant factor influencing nerve shear wave velocity outcomes. Ultrasound transducer positioning needs to be well controlled when using SWE to assess peripheral nerve’s integrity. It is important to note, however, that mechanical anisotropy may also be an interesting biomarker for peripheral nerve disorders characterized by structural disorganization.
Influence of Sex and Age on Nerve Shear Wave Velocity
There is limited evidence regarding the influence of age and sex on peripheral nerve shear wave velocity, including that of the sciatic and tibial nerves. One study measuring the shear wave velocity of the median and tibial nerves observed that male participants had significantly higher shear wave velocities for the median nerve than female participants, but no differences were observed regarding the tibial nerve [43]. Similar findings were reported in another study [42] that observed no differences in the stiffness of the tibial nerve between male and female participants. Conflicting results have been reported on the effect of ageing on nerve shear wave velocity. One study found higher values of stiffness in the tibial nerve of older participants compared to younger participants. However, the sample in this study was relatively young, with only three participants above 60 years old, versus 47 participants below 60 years, which limits the validity of conclusions about the influence of ageing on nerve stiffness. Other studies observed the opposite tendency, with shear wave velocity decreasing with age, both for the tibial [37] and the sciatic [39] nerves. This may be explained by age-related reductions in the thickness and in the content of collagen fibril of the sciatic nerve’s perineurium, as shown in animal studies [57]. Further studies are required to investigate the influence of demographic variables more comprehensively on peripheral nerve shear wave velocity, including their possible interactions with nerve regions and different tensile loads.
Additional Factors Influencing Nerve Shear Wave Velocity
The type of ultrasound scanner and the measurement depth are additional variables that can further impact normal shear wave velocity values and introduce variability when comparing across studies. For example, one study [58] reported significant differences in shear wave velocity obtained from ultrasound equipment from different manufacturers, using the same type of transducer and measuring at similar depths in an elasticity phantom. Another study reported different shear wave velocities from different ultrasound equipment when a soft elasticity phantom was used, but not with a harder phantom [59]. These small variations might be attributed to differences in the methodological procedures or computations used to estimate shear wave velocity among different manufacturers, potentially impacting the establishment of generalized cutoff values for various nerve-related disorders. Moreover, measuring shear wave velocity at depths ranging from 2 to 5 cm has also been shown to produce different results when using the same SWE scanner and transducer [58,60], with a trend for shear wave velocity to decrease in deeper regions [58]. As these results were mostly obtained from elasticity phantoms, it is important to determine whether these observations extend to the measurement of peripheral nerves, to improve the validity of nerve SWE assessments and its diagnostic value. However, the sciatic and tibial nerves are generally assessed at depths inferior to 3.5 cm, which might be covered by the focal area of linear probes typically used for these assessments.
Limitations of the Review
The current review presents some limitations. Other lower limb nerves, such as the fibular, femoral, obturator, and saphenous nerves, were not considered. However, elastography-based studies evaluating these nerves are scarce or even non-existent. Therefore, the primary focus of this review was on the most frequently assessed nerves—the sciatic and the tibial. Another potential limitation is the non-inclusion of clinical populations, where nerve mechanical properties have been shown to be considerably altered. This review exclusively considered healthy individuals, as we believe that it is crucial to first establish a comprehensive understanding of shear wave velocity in structurally and functionally intact tibial and sciatic nerves. By taking this approach, it is possible to carefully examine the potential factors that may influence these shear wave velocity measurements before thoroughly investigating their clinical applicability in serial and multi-center settings. Finally, the high variability in the methods used to measure nerve stiffness made it impossible to pool the results, leading us to the decision not to perform a meta-analysis.
Conclusion
Ultrasound SWE has been recognized as a valid and accurate non-invasive imaging technique for evaluating the mechanical properties of peripheral nerves, with shear wave velocity serving as a surrogate marker for nerve stiffness. In this systematic review, we compiled a comprehensive range of normal shear wave velocity values for both the sciatic and tibial nerves in healthy adults. This contributes to summarizing normative reference values to which shear wave velocity from diseased nerves can be compared. Importantly, we also identified the main factors directly influencing SWE assessments in peripheral nerves. Better understanding and accounting for spatial variations in nerve shear wave velocity, the intrinsic mechanical anisotropy of nerves, and the implication of limb postures on axial stretching is paramount to enhance the clinical applicability of SWE and compare outcomes across research studies. Standardized assessment protocols are required and need to take into consideration variables such as scanning postures, transducer orientation, and the nerve regions under assessment, as these factors are likely to directly and significantly affect nerve shear wave velocity. The pursuit of such standardization holds substantial promise for the advancement of clinical diagnosis and the monitoring of peripheral neuropathies using SWE. Consensus among expert practitioners (e.g., a Delphi study) is required to guide decision-making in the acquisition, analysis, and interpretation of SWE in peripheral nerves in experimental and clinical settings.
 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI



