Radiofrequency ablation of benign thyroid nodules: recommendations from the Asian Conference on Tumor Ablation Task Force
Article information

Abstract
Radiofrequency ablation (RFA) is a thermal ablation technique widely used for the management of benign thyroid nodules. To date, five academic societies in various countries have reported clinical practice guidelines, opinion statements, or recommendations regarding the use of thyroid RFA. However, despite some similarities, there are also differences among the guidelines, and a consensus is required regarding safe and effective treatment in Asian countries. Therefore, a task force was organized by the guideline committee of the Asian Conference on Tumor Ablation with the goal of devising recommendations for the clinical use of thyroid RFA. The recommendations in this article are based on a comprehensive analysis of the current literature and the consensus opinion of the task force members.
Introduction
Ultrasound (US)-guided radiofrequency ablation (RFA) is an alternative to surgery for patients with benign thyroid nodules [1-7]. Since 2001, many studies, including randomized controlled trials and meta-analyses, have reported the effectiveness and safety of this approach, resulting in its widespread use in patients with benign thyroid nodules [8-12]. Since the first recommendations of the Korean Society of Thyroid Radiology (KSThR) in 2009, academic societies in Italy, the United Kingdom, and Austria have established their own clinical practice guidelines, opinion statements, or recommendations for thyroid RFA [3-6]. Currently, the revised 2017 guidelines of the KSThR serve as the standard [2].
Despite some similarities, there are also differences among the clinical practice guidelines [2-6,13,14]. In addition, controversies exist that may be confusing for clinicians performing RFA [13]. Therefore, the guideline committee of the Asian Conference on Tumor Ablation (ACTA) organized a task force to devise recommendations for the use of RFA in the management of benign thyroid nodules. A systematic search of international databases, including MEDLINE and Embase, was performed using the keywords "thyroid" AND ("radiofrequency ablation" OR "RF ablation" OR "RFA") AND ("guideline" OR "recommendation" OR "opinion" OR "statement"). The search was limited to studies published in English between January 1, 2000 and August 2, 2019. Studies or subsets of studies that satisfied the following criteria were included: (1) population and intervention: benign thyroid nodules and image-guided RFA; (2) study design: clinical practice guidelines (opinion statement, recommendations, or guidelines); (3) outcomes: indications, preprocedural and postprocedural evaluation techniques and informed consent. In addition, an up-to-date search was conducted with the aim of answering some key questions. Based on a comprehensive analysis of the current literature, we generated online communications. Tables 1-3 describe the scope of the guidelines, methodology, and general information. The purpose of the recommendations is to provide a consensus expert opinion, based on the best scientific evidence available, to guide members of the ACTA in the use of thyroid RFA for the safe and effective management of benign thyroid nodules.
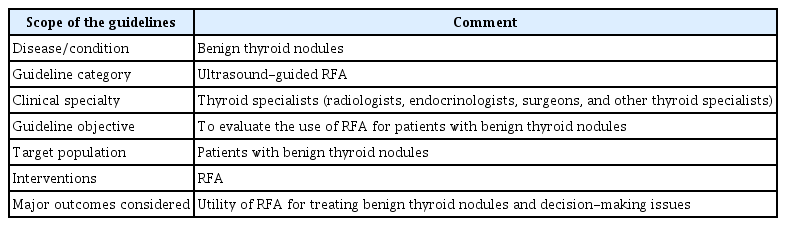
Scope of the guidelines

Methodology
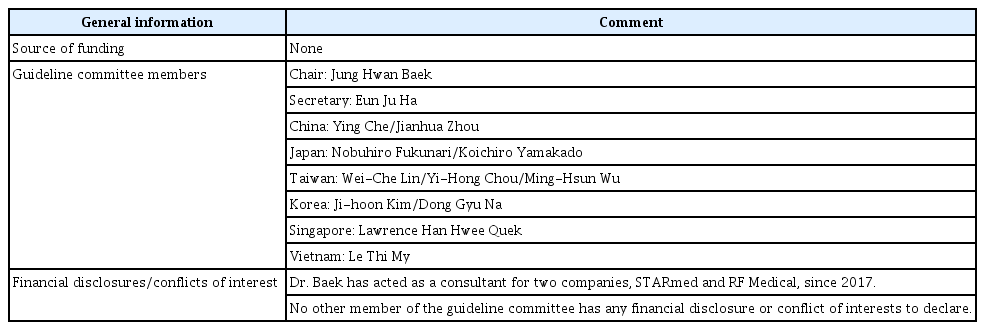
General information
Methodology
Following a review of the existing literature, a grading system was established based on the quality of evidence, clinical benefits and harms, costs, and patient preferences [15-17]. The modified Delphi method was used to formulate the recommendations, particularly regarding benefits and harms [17].
The committee comprised 13 experts in thyroid interventions, collectively representing six Asian countries. The level of evidence and benefit to patients were the main factors underlying the recommendations. The clinical applicability was discussed, as well as the impact of the recommendations on patient outcomes. Despite a high Delphi score, the recommendations were downgraded based on the consensus opinion of the committee.
Indications
Key question 1: What are the indications for RFA of benign, nonfunctioning thyroid nodules?
Recommendation 1
RFA is indicated for patients with benign, nonfunctioning thyroid nodules with symptoms or cosmetic issues.
For benign, nonfunctioning thyroid nodules, RFA should be restricted to patients with symptoms or cosmetic issues. Although the majority of benign thyroid nodules are asymptomatic and treatment is generally not required, some patients require treatment due to symptoms such as dysphagia, throat discomfort, foreign body sensation, pain, anterior neck mass, and cough, as well as for cosmetic reasons. Therefore, the purpose of RFA for benign, nonfunctioning thyroid nodules is to relieve symptoms and address cosmetic issues. A symptom score of 0-10 is generated using a 10-cm visual analog scale. A cosmetic score of 1-4 is derived by a physician, as follows: 1, no palpable mass; 2, no cosmetic issues but a palpable mass; 3, cosmetic issue only during swallowing; 4, nodule visible to the naked eye.
Debate and consensus
No definitive cutoff values are available for the size of benign thyroid nodules suitable for RFA. Most guidelines emphasize the importance of the patient’s symptoms and cosmetic concerns when making a clinical decision regarding RFA. Although large thyroid nodules often cause symptoms and cosmetic issues, the patient’s neck circumference and the location of the thyroid nodules are critical factors. The KSThR guidelines recommend that RFA can be considered for growing nodules >2.0 cm in size [2]. Italian guidelines also recommend RFA for nodules >2.0 cm in size [3,4]. Although there are no absolute contraindications for RFA, thyroid nodules showing retrosternal extension or extension into the Zuckerkandl tubercle can be difficult to access and multiple treatment sessions may be required. The use of a bipolar electrode can be recommended for pregnant women or patients with electrical devices, such as a cardiac pacemaker [18-20].
Key question 2: What are the indications for RFA in patients with autonomously functioning thyroid nodules (AFTNs)?
Recommendation 2
RFA may be indicated for AFTNs that are either toxic or pretoxic.
Although radioactive iodine (RAI) therapy and surgery are effective and relatively safe treatment options, hypothyroidism after surgery and RAI therapy may exacerbate pre-existing chronic conditions in the elderly and its use is also controversial in young women. Moreover, some patients refuse RAI therapy or surgery because of concerns regarding radiation exposure and potential complications, such as hypothyroidism. RFA can serve as an alternative treatment option for patients who refuse, or cannot undergo, traditional treatments, such as RAI or surgery, as well as for patients with a favorable condition, such as a small single AFTN [11,21-23].
Debate and consensus
Regarding the size of AFTNs considered suitable for RFA, all guidelines agree that small AFTNs can be effectively treated by a single session of RFA, with preservation of normal thyroid tissue function. However, some guidelines suggest that RFA may be less effective for large (volume >15-20 mL) or multifocal ATFNs [3-5]. The Italian guidelines recommended combined RFA and RAI treatment for large ATFNs (volume >20 mL) for more rapid improvement of local symptoms [3,4]. Recent meta-analyses have suggested that thermal ablation of AFTNs is an option regardless of nodule size. However, treatment efficacy may be lower in larger nodules and multiple sessions of RFA may be necessary [11,24]. Based on thyroid-stimulating hormone (TSH) normalization, no significant difference in the treatment response rate was seen between nodules with a volume ≤18 and >18 mL (73.6% vs. 67.0%, respectively; P=0.53) [24]. Regarding the number of treatment sessions, single and multiple sessions of RFA achieved TSH normalization in 66.7% and 79.3% of cases, respectively (P=0.23) [24]. The majority of the ACTA committee members agreed that RFA could be indicated for AFTNs regardless of nodule size. However, if clinical success (defined as TSH normalization) is likely to be difficult to achieve with one session (e.g., in cases of large nodule size, multifocality, or poor localization), RAI therapy with or without RFA or surgery may be considered first, instead of RFA. Multiple RFA sessions could be an option if patients refuse or cannot undergo surgery or RAI therapy in these situations. This issue should be evaluated further in future studies.
Preprocedural Evaluation
Key question 3: How can we confirm that thyroid nodules are benign before the procedure?
Recommendation 3.1
Thyroid nodules should be confirmed as benign on the basis of at least two US-guided fine-needle aspirations (FNAs) or core needle biopsies (CNBs) prior to RFA.
Before the procedure, thyroid nodules should be confirmed as benign on at least two FNAs or CNBs. Two benign biopsy results are required to prevent a possible false-negative diagnosis of malignancy (typically follicular carcinoma or follicular variant papillary thyroid carcinoma). However, even if thyroid nodules are confirmed to be benign, RFA should be performed carefully when there are suspicious US features.
Recommendation 3.2
A benign diagnosis based on a single FNA or CNB is sufficient when the nodule has US features highly suggestive of benign status (spongiform or partially cystic nodules with an intracystic comet tail artifact) and for AFTNs.
Debates and consensus
According to the KSThR guidelines, a single benign diagnosis is sufficient for thyroid nodules with US features highly suggestive of benign nodules (isoechoic spongiform or partially cystic nodules with an intracystic comet tail artifact) and for AFTNs [2]. Similarly, the Italian guidelines accept a single benign diagnosis for thyroid nodules shown by US to be entirely spongiform or ovoid, smooth, and isoechoic/hyperechoic, and for AFTNs [3,4]. Although US-based risk stratification systems differ among countries, we consider a single benign biopsy result to be acceptable for RFA of American College of Radiology (ACR) TR-1 nodules (spongiform), European Thyroid Imaging Reporting and Data System (EU-TIRADS) category 2 nodules (spongiform), American Association of Clinical Endocrinologists/American College of Endocrinology and Associazione Medici Endocrinologi (AACE/ACE-AME) low-risk nodules (spongiform and mostly cystic, with intracystic comet tail artifacts), and KSThR Thyroid Imaging Reporting and Data System (K-TIRADS) category 2 (spongiform or partially cystic with intracystic comet tail artifacts) nodules, given the very low risk of malignancy (typically <1%) [25-28]. However, although they are almost always benign when there is no co-occurring suspicious US feature for malignancy, a cautious approach is necessary to reduce the possibility of a false-negative diagnosis. On the contrary, follicular and follicular variant papillary thyroid carcinomas often show US features corresponding to ACR TR-2 (partially cystic isoechoic nodules without suspicious US features), EU-TIRADS category 3 (entirely isohyperechoic), AACE/ACE-AME intermediate-risk, American Thyroid Association Thyroid Imaging, Reporting and Data System very low-risk (partially cystic without suspicious US features), or K-TIRADS category 3 (isoechoic or partially cystic without suspicious US features) nodules [15,25-28]. Therefore, at least two benign biopsy results are necessary for these nodules before considering RFA, even though the risk may be low (approximately 2%-5%). Nodule selection for RFA should be decided based on a consensus between the patient and the clinician, who can evaluate the therapeutic options based on the patient’s best interests.
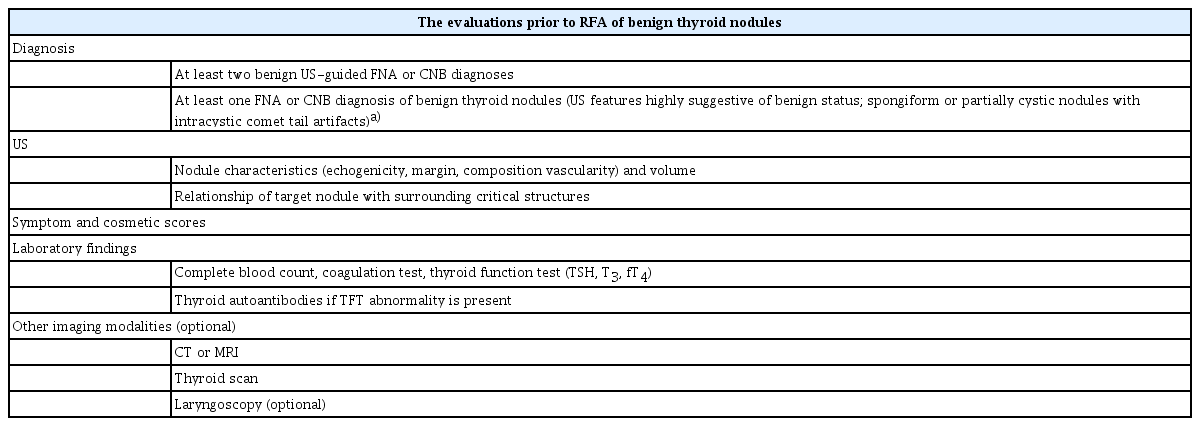
Table 4 lists the evaluations performed prior to RFA of benign thyroid nodules. The US features of thyroid nodules and patients’ symptom/cosmetic scores should be carefully considered. Nodule size, echogenicity, margin, solid component (%), internal vascularity and cervical lymph nodes should be evaluated in detail by US. The orthogonal diameter should be measured three times; the volume of the thyroid nodule should also be measured at baseline. Laboratory tests should include a complete blood count, coagulation test (bleeding, prothrombin, and activated partial thromboplastin times), and thyroid function test. The thyroid function test should include at least triiodothyronine (T3), triiodothyronine, and free thyroxine (fT4). Hypothyroidism should be addressed by hormone replacement therapy, and hyperthyroidism should be further evaluated by a technetium 99mTc pertechnetate or 123I thyroid scan. A thyroid function test is important to evaluate the treatment outcome of patients with AFTNs, where remission or normalization of thyroid function can be considered to indicate successful ablation. Autoantibodies (anti-thyroid peroxidase and anti-thyroglobulin antibodies) can be selectively measured in some cases. Computed tomography or magnetic resonance imaging may be useful to assess nodules for suspected intrathoracic extension and tracheal compression. A laryngoscopic examination to evaluate vocal cord status is not routinely recommended prior to RFA. However, a laryngoscopic examination is necessary for patients with suspected vocal cord paralysis. US evaluation of the larynx can be effective for the patients with no history of hoarseness. Any prescribed medications that can cause bleeding should be discontinued prior to RFA (7-10 days for aspirin or clopidogrel, 3-5 days for warfarin, and 4-6 hours for heparin). Patients can resume their medication after RFA (2-6 hours for heparin, the following night for warfarin, and the following day for aspirin or clopidogrel) [29].
Preprocedural checklist for radiofrequency ablation of benign thyroid nodules
Procedure
Key question 4: What is the most appropriate technique for RFA of benign thyroid nodules?
Recommendation 4.1
Perithyroidal lidocaine injection is recommended for local anesthesia.
We recommend a perithyroidal lidocaine injection to reduce pain during the procedure, as sensory nerves are usually present along the thyroid capsule. However, a direct injection of lidocaine into the region of the recurrent laryngeal nerve is not recommended during the procedure, in order to avoid voice changes [2-6].
Debate and consensus
Considering the balance between benefits and harms, general anesthesia is not recommended. For example, early detection of major complications, such as nerve damage or tracheal injury, may not be possible under general anesthesia. However, conscious sedation is a potential option for nervous patients or those with special clinical concerns. A recent paper reported that nerve damage could be effectively managed by injecting cold 5% dextrose water (DW) into the area surrounding the damaged nerve [30]. In cases where conscious sedation is required, RFA should be performed carefully to avoid complications, particularly by sparing areas near the critical structures, including the recurrent laryngeal nerve, cervical sympathetic ganglion, and vagus nerve, that are vulnerable to thermal injury [10,31,32].
Recommendation 4.2
A trans-isthmic approach and the moving-shot technique are recommended as standard.
The trans-isthmic approach and moving-shot technique are fundamental for safe and effective RFA. In the trans-isthmic approach, the electrode needle is inserted via the thyroid isthmus in the midline-to-lateral direction. This technique has several advantages: first, the entire length of the electrode can be visualized; secondly, exposure of the danger triangle to heat can be minimized; and thirdly, movement of the electrode is minimized during swallowing and talking. After insertion of the electrode using the trans-isthmic approach, RFA is performed using the moving-shot technique. The moving-shot technique was developed specifically for the thyroid gland, as thyroid nodules are ellipsoidal and exophytic to the thyroid gland, but lie close to many critical structures such as the esophagus, trachea, recurrent laryngeal nerve, vagus nerve, cervical sympathetic ganglion, and carotid artery. This technique involves dividing the thyroid nodule into multiple small ablation units, which are then ablated by moving the electrode around. The electrode is inserted at the deepest and most remote portion of the target nodule, and is then moved backward as the needle is gradually withdrawn [33].
Advanced techniques, including vascular ablation and hydrodissection, have recently been introduced for thyroid RFA [2,34]. Vascular ablation includes two different techniques: artery-first ablation and marginal venous ablation. These techniques can reduce marginal recurrence in cases with hypervascular nodules. Hydrodissection can preserve a safety margin around adjacent critical structures during RFA. In this technique, 5% DW is injected to separate the thyroid nodules from many critical structures; the nodule margin can then be treated safely using the 5% DW as a thermal barrier [2,35,36].
Postprocedural Evaluation
Following RFA, all clinical, imaging, and laboratory findings should be re-evaluated. The ultimate goal of RFA is clinical success, which is defined as the resolution of clinical problems (i.e., symptoms and cosmetic issues in patients with nonfunctioning nodules and thyroid function test normalization in patients with AFTN) [39]. We generally recommend that follow-up visits be scheduled for 1, 6, and 12 months, and every 6-12 months thereafter, according to the status of the treated nodule. As the successful treatment of nonfunctioning benign thyroid nodules is dependent on improving symptoms and cosmetic issues by reducing nodule volume, US findings, as well as symptom and cosmetic scores, should be evaluated after RFA and compared with previous scores. On follow-up US images, physicians should evaluate the nodule size and volume, echogenicity, and internal vascularity. The volume reduction rate (VRR) can be calculated as follows: (initial volume-final volume)×100/initial volume. Regular thyroid function test follow-up is not routinely recommended after treatment of nonfunctioning benign thyroid nodules; however, it is necessary for patients with clinical symptoms of thyroid function abnormality or US suspicion of diffuse thyroid disease prior to RFA.
Following RFA for AFTNs, thyroid function tests that measure TSH, T3, and fT4 should be carried out; thyroid scans can also be helpful to determine the therapeutic response. In patients with elevated thyroid antibodies prior to RFA, careful evaluation of the thyroid function test is necessary, as some patients may exhibit hypothyroidism following treatment.
Key question 5: When should additional treatment be considered after RFA?
Recommendation 5
Additional treatment is recommended when the treated nodule shows marginal regrowth or <50% volume reduction, and when there is incomplete resolution (or relapse) of symptoms/cosmetic issues.
Debate and consensus
The indications for additional RFA have not yet been fully defined. However, we recommend additional RFA in the following scenarios: marginal regrowth of the treated nodule (which is defined as nodule volume increase of ≥50% compared to the minimum recorded volume measured at a given follow-up time point), <50% VRR, and incomplete resolution (or relapse) of symptoms or cosmetic issues [2-4,39]. When the nodule shows vascularity or a volume increase during follow-up, additional ablation should be carefully considered [40]. Regarding AFTNs, the decision for additional treatment is based on the serum TSH level [2,3,39].
Safety
Key question 6: Is RFA a safe procedure?
Recommendation 6
RFA is a safe procedure when performed by experienced operators.
Previous guidelines and studies, including meta-analyses, have shown that RFA is a safe procedure for the treatment of benign thyroid nodules and has a low incidence of complications [10,31]. The overall complication rate was reported as 2.11% (95% confidence interval [CI], 1.15 to 3.06) and the major complication rate was 1.27% (95% CI, 0.81 to 1.73) [10]. Previous studies have shown that RFA performed by trained radiologists, using a unified protocol and similar devices, is safe for treating benign thyroid nodules. They defined an experienced operator as one who has successfully completed >50 thyroid RFAs [12].
However, complications associated with RFA have been reported, including major complications such as nerve injury (including the recurrent laryngeal nerve, cervical sympathetic ganglion, vagus nerve, and brachial plexus), nodule rupture, and permanent hypothyroidism [10,31]. Minor complications may include hematoma, vomiting, skin burn, transient thyrotoxicosis, lidocaine toxicity, hypertension, and pain [10,31]. There are no known life-threatening complications, and the sequelae rate was reported to be only 0.21%. A thorough knowledge of neck anatomy and its clinical significance is essential for the safe and effective use of US-guided procedures [32,41,42].
Conclusion
These are the first thyroid RFA guidelines developed by an international academic society. They are based on an analysis of the similarities and differences among five guidelines from different countries and the expert opinion of the ACTA taskforce members. Unresolved issues in these guidelines require further evaluation and discussion.
Notes
Author Contributions
Conceptualization: Baek JH, Ha EJ. Drafting of the manuscript: Baek JH, Ha EJ. Critical revision of the manuscript: Ha EJ, Baek JH, Che Y, Chou YH, Fukunari N, Kim JH, Lin WC, My LT, Na DG, Quek LHH, Wu MH, Yamakado K, Zhou J. Approval of the final version of the manuscript: all authors.
Dr. Baek has acted as a consultant for two companies, STARmed and RF Medical, since 2017. No other member of the guideline committee has any financial disclosure or conflict of interests to declare.