Sonazoid-enhanced ultrasonography for noninvasive imaging diagnosis of hepatocellular carcinoma: special emphasis on the 2022 KLCA-NCC guideline
Article information

Abstract
Contrast-enhanced ultrasonography (CEUS) is a noninvasive imaging modality used to diagnose hepatocellular carcinoma (HCC) based on specific imaging features, without the need for pathologic confirmation. Two types of ultrasound contrast agents are commercially available: pure intravascular agents (such as SonoVue) and Kupffer agents (such as Sonazoid). Major guidelines recognize CEUS as a reliable imaging method for HCC diagnosis, although they differ depending on the contrast agents used. The Korean Liver Cancer Association–National Cancer Center guideline includes CEUS with either SonoVue or Sonazoid as a second-line diagnostic technique. However, Sonazoid-enhanced ultrasound is associated with several unresolved issues. This review provides a comparative overview of these contrast agents regarding pharmacokinetic features, examination protocols, diagnostic criteria for HCC, and potential applications in the HCC diagnostic algorithm.
Introduction
Hepatocellular carcinoma (HCC) primarily affects patients with chronic liver disease, and a noninvasive diagnosis can be performed in high-risk patients using cross-sectional imaging techniques such as computed tomography (CT), magnetic resonance imaging (MRI), and contrast-enhanced ultrasonography (CEUS) [1]. Several guidelines have incorporated CEUS as a key imaging modality for the noninvasive diagnosis of HCC, including those from the American Association for the Study of Liver Diseases, the European Association for the Study of the Liver (EASL), the Asian Pacific Association for the Study of the Liver (APASL), the Japan Society of Hepatology (JSH), and the Korean Liver Cancer Association–National Cancer Center (KLCA-NCC) [2-7]. Furthermore, the CEUS Liver Imaging Reporting and Data System (CEUS LI-RADS) diagnostic algorithm was created to standardize the acquisition, interpretation, and reporting of CEUS studies for HCC diagnosis [8].
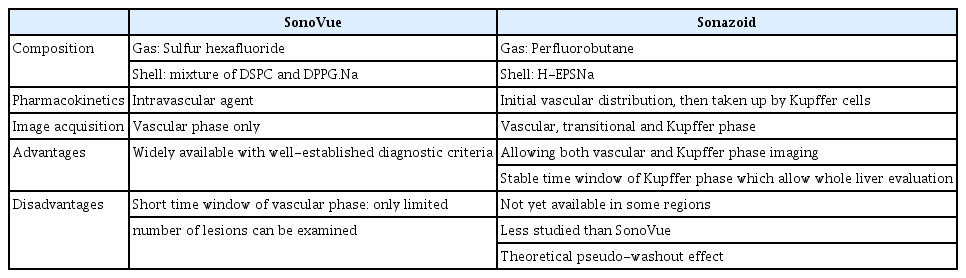
Currently, two types of ultrasound contrast agents (UCAs) are commercially available: (1) pure intravascular agents, such as SonoVue (Bracco Diagnostics, Milan, Italy) or Definity (Lantheus Medical Imaging, Billerica, MA, USA), and (2) Kupffer agents, such as Sonazoid (GE Healthcare, Oslo, Norway) [9]. The key difference between Kupffer agents and intravascular agents is that the former are phagocytosed by Kupffer cells in the liver. CEUS with intravascular agents was included in the EASL and 2018 KLCA-NCC guidelines, as well as the CEUS LI-RADS, while CEUS with Kupffer agents was included in the APASL and JSH guidelines [4,6-8]. More recently, the 2022 KLCA-NCC guideline has incorporated CEUS with either contrast agent as a secondary diagnostic modality [3]. This review discusses Sonazoid-enhanced ultrasound (SZUS) and compares it to SonoVue-enhanced ultrasound (SVUS) in terms of pharmacokinetic features, examination protocols, diagnostic criteria for HCC, and potential applications in the HCC diagnostic algorithm.
Pharmacokinetic Properties of UCAs
UCAs are composed of a suspension of bubbles with diameters ranging from 2-5 µm (i.e., smaller than a red blood cell) [10]. Three second-generation UCAs are commercially available: SonoVue, Definity, and Sonazoid. The first two are purely intravascular agents, with only SonoVue being commercially available in Korea. In contrast, Sonazoid is a combined intravascular and Kupffer cell agent [9]. SonoVue and Sonazoid exhibit different pharmacokinetic properties. After intravenous injection, SonoVue remains in the blood vessels, reaching its maximum concentration within 1-2 minutes following a single administration. It then dissolves as sulfur hexafluoride gas in the blood and is rapidly eliminated through expired air within 10 minutes [9]. Sonazoid consists of microbubbles of perfluorobutane encapsulated in a shell of hydrogenated egg phosphatidylserines, with an average size of 2.6 µm. Like SonoVue, Sonazoid remains in the blood vessels and is then taken up by Kupffer cells (starting approximately 1 minute after administration). The maximum concentration of Sonazoid in the vessels is observed 1 to 2 minutes after intravenous administration [11,12]. Its blood elimination half-life is approximately 20-35 minutes, with most of the agent eliminated through the lungs [11,12]. The characteristic feature of Sonazoid is its accumulation in the reticuloendothelial system, such as the Kupffer cells present in the liver parenchyma [13,14]. Sonazoid microbubbles provide prolonged enhancement of the liver parenchyma for up to 2 hour post-injection via Kupffer cell phagocytosis (Kupffer phase or post-vascular phase) [15]. Detailed information on the characteristics of each agent, along with technical requirements, is presented in Table 1.
Differences between SonoVue and Sonazoid for HCC diagnosis
Imaging Acquisition Technique
Image acquisition for CEUS involves real-time imaging conducted at frame rates of approximately 10 frames per second, offering the highest temporal resolution currently available for liver imaging [16]. Typically, a single injection is used to focus on one nodule, with the transducer remaining in a fixed position throughout at least the arterial phase and often the entire scan [16]. A CEUS examination employs contrast-specific imaging techniques, such as phase or amplitude modulation, and typically utilizes a low mechanical index (MI). However, SZUS employs a higher MI (≤0.25) than SVUS (MI ≤0.15). This primary technical distinction between the two agents is largely due to Sonazoid’s increased resistance to acoustic pressure [10].
SonoVue
Typically, the dose of SonoVue ranges from 1.5 to 2.4 mL, administered as a bolus injection followed by a 5- to 10-mL saline flush. However, equipment-, transducer-, and patient-specific factors may necessitate adjustments to these parameters [16]. Generally, three phases of vascular enhancement can be observed in CEUS with SonoVue: (1) the arterial phase, occurring from 10 to 20 seconds up to 45 seconds post-injection; (2) the portal venous phase, taking place from 30 to 50 seconds up to 2 minutes post-injection; and (3) the late phase, lasting from 2 minutes until microbubble clearance, approximately 5 minutes post-injection (Fig. 1) [9,17]. Continuous scanning and recording are recommended until 70 seconds after the saline flush in order to evaluate the enhancement pattern during the arterial phase and document early washout (<60 seconds). Following this, intermittent imaging at 15- to 20-second intervals is advised until washout becomes apparent. The degree of washout should be assessed at 2 minutes post-injection. If washout is not clearly visible, intermittent imaging should continue until microbubbles have been cleared from the circulation (approximately 5 minutes post-injection) [16].

Phases of contrast-enhanced ultrasonography.
A. SonoVue-enhanced ultrasonography illustrates the vascular phase, which consists of arterial, portal, and late phases. Images can be viewed until microbubbles are cleared from circulation, approximately 5 minutes after contrast injection. B. Sonazoid-enhanced ultrasonography displays both the vascular phase and the post-vascular phase. The vascular phase includes arterial, portal, and transitional (vasculo-Kupffer) phases. The uptake of microbubbles by Kupffer cells begins approximately 1 minute after contrast injection. As a result, the enhancement following the portal phase may represent a combination of the vascular and Kupffer phases. The Kupffer phase is regarded as a post-vascular phase.
Sonazoid
Generally, the recommended dosage of Sonazoid is 0.015 mL/kg. However, due to recent advancements in CEUS techniques that have increased sensitivity for microbubbles, half to two-thirds of the dose per individual is also commonly used [18]. With Sonazoid, the arterial phase resembles that of SonoVue and can be observed from 10-20 seconds to 45 seconds after injection. However, 1-2 minutes post-injection, the liver enhancement pattern may be similar but not identical to that of SVUS, since Kupffer cell uptake begins approximately 1 minute after administration [15,19]. As a result, the enhancement observed after the portal venous phase may represent a combination of the vascular and Kupffer phases (transitional phase or vasculo-Kupffer phase) [19,20]. The pure Kupffer phase (also known as the post-vascular phase) starts at approximately 10 minutes post-injection, when the microbubbles have been eliminated from the blood pool, and lasts up to 2 hours (Fig. 1) [9,10,15]. As with SVUS, continuous scanning and recording are recommended until 70 seconds after saline flushing to evaluate the enhancement pattern in the arterial phase and document early washout. This should be followed by intermittent imaging at 15- to 20-second intervals until washout appears. The degree of washout should be assessed at 2 minutes post-injection. If washout is not evident, intermittent imaging is recommended until 5 minutes post-injection. Subsequently, Kupffer phase imaging can be obtained between 6 minutes and 120 minutes, but a 10-minute delayed scan is most commonly used [10,21].
Diagnostic Criteria for HCC Using SZUS
Arterial Phase Hyperenhancement
The density of unpaired arteries progressively increases during hepatocarcinogenesis [22]; therefore, arterial phase hyperenhancement (APHE) is an important imaging feature for diagnosing HCC in at-risk patients using CT/MRI and SZUS (Fig. 2). Specifically, non-rim and non-globular APHE are the primary imaging features for HCC, as rim APHE is a distinctive feature of non-HCC hepatic malignancies (Fig. 3) and peripheral globular enhancement is a characteristic feature of hemangioma (Fig. 4). In a study comparing CT/MRI LI-RADS with SZUS [23], 89.6% of CT/MRI LR-5 (definitely HCC) and 85.9% of LR-4 (probably HCC) cases exhibited non-rim and non-globular APHE on Sonazoid CEUS, while only 57.6% of LR-3 (intermediate probability of malignancy) cases showed the same. In two separate studies of at-risk nodules, the presence of non-rim and non-globular APHE was identified as a strong indicator of HCC. In the first study of 113 at-risk nodules [21], 86.8% (72/82) of HCC cases displayed non-rim and non-globular APHE, while only 56.2% (9/16) of non-HCC malignancies and 20% (3/15) of benign lesions exhibited the same. Similarly, a study of 59 at-risk nodules revealed that 95% (41/43) of HCC cases presented non-rim and non-globular APHE, while only 30% (3/10) of non-HCC malignancies and 16.7% (1/6) of benign lesions demonstrated these imaging features [24]. Additionally, the enhancement patterns of HCC in the arterial phase were consistent in an intra-individual comparison of SVUS and SZUS, potentially due to the purely intravascular nature of the arterial phase of SZUS, which has minimal effects on Kupffer cell uptake [24].
Typical Sonazoid-enhanced ultrasound findings of hepatocellular carcinoma.
A-C. A 3.4-cm mass (arrows) in liver segment 6 exhibits non-rim nonglobular arterial phase hyperenhancement (A) and late washout (91 seconds postcontrast) (B) with a mild degree at 2 minutes postcontrast (C). D. Hypoenhancement of the lesion (arrow) is observed in the Kupffer phase.
Typical Sonazoid-enhanced ultrasound findings of intrahepatic cholangiocarcinoma.
A. A 3.2-cm lesion in liver segment 8 exhibits rim arterial phase hyperenhancement (arrow). B, C. This lesion (arrows) demonstrates (B) early washout (48 seconds post-contrast) with (C) a marked degree at 2 minutes post-contrast image. D. This lesion shows hypoenhancement in the Kupffer phase (arrow).
Typical Sonazoid-enhanced ultrasound findings of hemangioma.
A. A 1.7-cm lesion in liver segment 5 displays peripheral globular enhancement (arrows) in the arterial phase. B, C. At 2 minutes (arrow, B) and 4 minutes (arrow, C) after contrast injection, this lesion exhibits hypoenhancement (arrow) compared to the adjacent hepatic parenchyma. D. In the Kupffer phase, this lesion demonstrates mild hypoenhancement (arrow). Other than the peripheral globular enhancement in the arterial phase (A), the imaging features resembled those of hepatocellular carcinoma (HCC). Therefore, it is important to carefully inspect and rule out hemangioma in the arterial phase to avoid false positive diagnoses for HCC.
Washout
During hepatocarcinogenesis, the portal triad diminishes, while the unpaired arteries expand [22]. This results in a washout appearance, which is characterized by a temporary reduction in enhancement compared to the liver parenchyma during the portal venous or delay phase [25]. This washout appearance is a key imaging feature for diagnosing HCC in at-risk patients using CT/MRI [3,25]. However, early studies of CEUS indicated that washout alone was insufficient to distinguish HCC from intrahepatic cholangiocarcinoma [26], as most malignancies consistently exhibit washout on CEUS due to the strict intravascular property of the contrast agent [27]. Subsequent research has shown that the timing and degree of washout are crucial factors in differentiating HCC from other solid focal liver lesions [28-30]. Specifically, late timing (≥60 seconds) and a mild degree of washout are the primary imaging features for distinguishing HCC from other malignancies on CEUS when using an intravascular agent [16].
In SZUS, the washout criteria for HCC diagnosis resemble those in CEUS with intravascular agents. The late and mild degree of washout is a major imaging feature of HCC, and the degree of washout should be evaluated at 2 minutes post-injection [20]. However, the unique characteristics of Sonazoid, which is phagocytosed by Kupffer cells, may cause a pseudo-washout effect. Therefore, a careful approach is needed to assess the washout. The key issues are the cutoff time to determine "late washout" and the time period to observe the washout. In a study suggesting washout criteria for HCC in SZUS [21], the specificity and positive predictive value were 100% when late washout was defined as 60 seconds or later in SZUS, and the peak timing of washout was 72-120 seconds, although 21% of HCCs showed mild washout before 60 seconds. The 60-second cutoff time to determine late washout was the same as the criteria for CEUS using an intravascular agent. This may be explained by the intravascular nature of the early vascular phase of SZUS, which has minimal effects on Kupffer cell uptake. Additionally, the time period during which to observe the washout requires a cautious approach due to the pseudo-washout effect. In a study of washout of SZUS on 116 at-risk nodules [21], the specificity did not change when observing the washout until 6 minutes post-injection compared to observation until 3 minutes post-injection. This result suggested that determining washout within 6 minutes post-injection with a 60-second cutoff for late washout is reliable for diagnosing HCC using SZUS in high-risk individuals.
Kupffer Phase Hypoenhancement
Kupffer cells are a specific type of macrophage found within the liver, comprising approximately 30% of sinusoidal cells [31]. Consequently, any condition that affects the sinusoidal structure can also alter the intralesional density of Kupffer cells and the echogenicity in the Kupffer phase. Hepatic tumors, including HCC, typically exhibit low intratumoral Kupffer cell density due to alterations in the blood space [32]. Previous studies [21,24,33] have shown that 87%-96% of HCCs and 90%-100% of non-HCC malignancies exhibit hypoenhancement in the Kupffer phase.
Moreover, the hypoenhancement of HCC in the Kupffer phase represents a highly sensitive imaging feature compared to washout [20]. Previous research has demonstrated that a small percentage (5% to 10%) of pathologically confirmed HCC cases exhibit hypoenhancement exclusively in the Kupffer phase, rather than in washout during the vascular phase [34,35]. This phenomenon is more commonly observed in early or well-differentiated HCCs [34,35]. As a result, detection of hypoenhancement in the Kupffer phase has the potential to identify HCC cases that might otherwise go undiagnosed based only on late and mild washout.
Numerous studies have sought to identify the optimal use of the Kupffer phase in diagnosing HCC. The key question is whether hypoenhancement in the Kupffer phase can function as an alternative or supplementary diagnostic criterion for washout. In a recent study by Hwang et al. [33], the diagnostic criteria for HCC incorporated APHE and Kupffer phase hypoenhancement while adjusting for grayscale findings (lesions with ill-defined margins without a hypoechoic halo were downgraded to non-HCC). These revised criteria demonstrated higher sensitivity without sacrificing specificity compared to the conventional criteria: non-rim APHE with late and mild washout. Additionally, Sugimoto et al. [36] reported satisfactory diagnostic performance, with 70.5% sensitivity and 92.5% specificity, for the following diagnostic criteria for HCC: nodules (≥1 cm) exhibiting APHE, no early washout, and hypoenhancement in the Kupffer phase.
In other applications, the Kupffer phase can be used to supplement washout in the diagnosis of HCC. In the study by Takahashi et al. [37], the inclusion of Kupffer phase detection as a major imaging feature in the conventional criteria for HCC diagnosis increased sensitivity from 52% to 67% without a significant loss of specificity. This approach can provide high specificity by considering washout features such as early or marked washout to differentiate HCC from non-HCC malignancies, highlighting the role of washout in SZUS. However, as previously mentioned, other hepatic tumors, such as hemangiomas, adenomas, or non-HCC malignancies, can also exhibit hypoenhancement in the Kupffer phase, which may lower specificity [24,38]. To differentiate these lesions, imaging features of the arterial phase and washout are crucial. Peripheral globular enhancement in the arterial phase is a characteristic feature of hemangiomas (Fig. 4). Rim APHE and early (<60 seconds) or marked washout are specific for malignancies other than HCC (Fig. 3). Therefore, through careful examination of the vascular phase, the Kupffer phase could contribute to improved diagnostic performance in HCC diagnosis.
Diagnostic Criteria for HCC
Among the various diagnostic criteria for SZUS, non-rim and non-globular APHE (≥1 cm) along with late (≥60 seconds) and mild washout are suitable major imaging features for diagnosing HCC in at-risk patients, as supported by several studies and illustrated in Fig. 2 [20,21,23,24,39]. This criterion is identical to conventional SVUS criteria [8,17]. Moreover, when a non-rim APHE lesion (≥1 cm) does not exhibit washout in the vascular phase, with careful examination of grayscale imaging features (such as an ill-defined margin without a hypoechoic halo, or globular or rim enhancement of the arterial phase to exclude hemangioma or non-HCC malignancy), hypoenhancement in the Kupffer phase can serve as an alternative and is considered a major imaging feature for diagnosing HCC in high-risk individuals to increase sensitivity. However, when the Kupffer phase alone is used to replace the washout phase, the specificity of HCC diagnosis will inevitably decrease because hemangiomas and non-HCC malignancies can also present with hypoenhancement in the Kupffer phase, as well as non-rim APHE [24,38]. Consequently, in several Asian countries where hepatic resection and ablation therapies are the primary options for treating early-stage HCC, a preference exists for maximal sensitivity in HCC diagnosis. As such, Kupffer phase hypoenhancement may be considered an acceptable alternative to washout [1]. In contrast, in North America and Europe, liver transplants are frequently used to manage early-stage HCC, and a high level of specificity in an HCC diagnostic algorithm is desired. Thus, Kupffer phase hypoenhancement may be employed as an ancillary imaging feature in these regions.
Diagnostic Performance of SZUS in HCC Diagnosis
In a recent intra-individual comparison between SVUS and SZUS [24], SZUS demonstrated greater sensitivity (54% vs. 79%) and accuracy (77% vs. 87%) than SVUS when using the same diagnostic criteria: non-rim APHE and late (≥60 seconds) and mild washout. While the enhancement patterns in the arterial phase did not significantly differ, the washout time for HCC was longer with SZUS than with SVUS (median, 101 seconds vs. 84 seconds, respectively). Additionally, a higher proportion of HCC was classified as LR-M in SVUS due to the increased occurrence of early washout (<60 seconds) [24]. However, that study had a small, single-center population, raising questions about its generalizability.
In a non-inferiority test of 105 at-risk hepatic nodules [39], the per-lesion accuracy of SZUS was found to be non-inferior to that of SVUS in diagnosing HCC in at-risk patients, using the same diagnostic criteria and meeting the statistical criterion for non-inferiority. In another non-inferiority test evaluating SZUS for characterizing focal liver lesions in high-risk individuals [40], SZUS was not inferior to SVUS for characterizing focal liver lesions and showed improved accuracy for both SZUS and SVUS, meeting the non-inferiority margin of -20%. Furthermore, no significant differences in adverse event rates were found between SVUS and SZUS [40].
Anticipated Role of CEUS in the Noninvasive Diagnosis of HCC According to the 2022 KLCA-NCC Guideline
The 2022 KLCA-NCC guideline recommends using CEUS with both SonoVue and Sonazoid as a second-line modality, due to the limited capability of CEUS in staging HCC. This approach is primarily employed when first-line examinations (such as CT or MRI) yield inconclusive results [3]. Unlike the iodine or gadolinium contrast agents used in CT or MRI, UCAs seldom disperse into the interstitial space because of their size. Furthermore, the real-time imaging capability of CEUS helps to reduce the mistiming issue associated with cross-sectional imaging (Fig. 5).
A 66-year-old man with pathologically confirmed hepatocellular carcinoma (HCC) in the liver.
A-C. On multiphase computed tomography (CT), a 1.5-cm mass (arrow) with non-rim non-globular arterial phase hyperenhancement (APHE) in liver segment 8 (A) exhibits equivocal washout in both portal (B) and delayed (C) phases (arrows, B and C). D-F. These CT imaging features are insufficient for a noninvasive HCC diagnosis. On Sonazoid-enhanced ultrasound, the mass displays APHE (arrow, D), late (160 seconds) and mild washout (arrow, E), and hypoenhancement (arrow, F) in the Kupffer phase. Consequently, this lesion could be noninvasively diagnosed as HCC.
Several studies have demonstrated that CEUS can increase sensitivity by revealing more APHE and/or washout when employed as a secondary modality for indeterminate lesions on CT/MRI, without compromising specificity [41-44]. Furthermore, perfusion abnormalities or pseudolesions, which frequently resemble genuine hepatic lesions on CT/MRI, are seldom visualized on CEUS. Consequently, CEUS is valuable for distinguishing true nodules from lesions when CT/MRI results are inconclusive [45].
Other SZUS-Related Issues
Several issues remain to be addressed, including (1) standardization of contrast dosage and acquisition protocol, (2) terminology for the phase between 1 minute and the Kupffer phase (10 minutes post-injection), and (3) a lack of consensus regarding the criteria for definitive HCC diagnosis. Of these, the most critical issue is the diagnostic criteria for HCC.
To date, the contrast dosage used in studies has been inconsistent, with some employing the vendor-recommended dose while others utilize a reduced dose (half-dose) [23,36,39,46,47]. Additionally, imaging acquisition methods have not been standardized, and images of late vascular or transitional phases may or may not be obtained [9,23,36,39,46,47]. Further research is needed to establish standardized contrast dosages and imaging acquisition protocols for SZUS, as has been done for SVUS.
Indeed, no consensus exists on the diagnostic criteria for HCC using SZUS. While the combination of APHE and hypoenhancement in the Kupffer phase of a hepatic lesion could offer high sensitivity, it may also result in low specificity [36,48]. In the 2022 KLCA-NCC guideline, the recommended criteria include APHE and mild/late washout or hypoenhancement in the Kupffer phase, after excluding peripheral globular enhancement, rim APHE, rapid washout within 60 seconds, or marked washout (punch-out appearance) within 2 minutes post-injection [3]. A recent study by Kang et al. [39] indicated that using these criteria, SZUS demonstrated non-inferior diagnostic performance to SVUS for diagnosing HCC. In theory, the additional enhancement of the liver parenchyma through Kupffer cell adhesion or phagocytosis of bubbles may occur during the vasculo-Kupffer or transitional phase with SZUS, potentially causing a pseudo-washout effect in focal liver lesions, such as flash-enhancing hemangioma [36,38]. However, since many intrahepatic cholangiocarcinomas exhibit either rim APHE or rapid/marked washout, this pseudo-washout effect may not pose significant issues. Recent studies by Kang et al. [24,39] and Sugimoto et al. [36], reported no cases of intrahepatic cholangiocarcinoma exhibiting pseudo-washout effects. Nevertheless, these findings should be validated through a multicenter prospective study involving a larger patient population.
In 2022, the KLCA-NCC Korean practice guideline for HCC incorporated SZUS as a second-line diagnostic test. Numerous studies have shown the value of CEUS as a second-line approach for enhancing sensitivity without sacrificing specificity. However, considerable differences in the diagnostic criteria of SZUS for HCC currently exist among the KLCA-NCC, JSH, and APASL guidelines. To establish a consistent set of diagnostic criteria for CEUS in diagnosing HCC, further large-scale, multicenter prospective studies are required. Moreover, the development of standardized terminology, contrast dosage, and imaging acquisition methods is crucial for advancing the use of CEUS as a noninvasive diagnostic tool for HCC.
Conclusion
Sonazoid is phagocytosed by Kupffer cells, allowing the visualization of the Kupffer phase. SZUS comprises arterial, portal venous, transitional, and Kupffer phases. The diagnostic criteria for HCC in SZUS are quite similar to those in SVUS; however, the addition of the Kupffer phase can increase the sensitivity for HCC diagnosis. Consequently, SZUS is a valuable second-line imaging modality for noninvasive HCC diagnostic algorithms.
Notes
Author Contributions
Conceptualization: Kang HJ, Lee JM. Data acquisition: Kang HJ, Lee JM. Data analysis or interpretation: Kang HJ, Lee JM, Kim SW. Drafting of the manuscript: Kang HJ, Lee JM, Kim SW. Critical revision of the manuscript: Kang HJ, Lee JM. Approval of the final version of the manuscript: all authors.
No potential conflict of interest relevant to this article was reported.
References
Article information Continued
Notes
Key point
Sonazoid is phagocytosed by Kupffer cells, allowing visualization of the Kupffer phase. The diagnostic criteria for hepatocellular carcinoma (HCC) in Sonazoid-enhanced ultrasound (SZUS) closely resemble those in SonoVue-enhanced ultrasound, and the Kupffer phase can be utilized for increased sensitivity. SZUS serves as a valuable second-line imaging modality for diagnosing noninvasive HCC.