Ultrasonographic diagnosis of round ligament varicosities mimicking inguinal hernia: report of two cases with literature review
Article information

Abstract
Round ligament varicosities are rare, and the mass mimics an inguinal hernia. Round ligament varicosities should be considered in the differential diagnosis of a groin swelling in a female, especially during pregnancy. The diagnosis of round ligament varicosities can be established on grayscale and color Doppler ultrasonography. We report two cases of round ligament varicosities in a 33-year-old non pregnant woman and a 28-year-old pregnant woman, and these patients were diagnosed using ultrasonography. We also reviewed the literature on round ligament varicosities including the present cases. Ultrasonography is diagnostic and can prevent unnecessary surgical intervention and associated morbidity.
Introduction
Round ligament varicosities (RLVs) have not been widely reported, and all cases have been described during pregnancy to the best of our knowledge [1-4]. The swelling mimics an inguinal hernia and should be considered in the differential diagnosis of a groin swelling, especially during pregnancy. A clinical distinction between the two disease entities is difficult. Unnecessary surgical intervention and associated morbidity is a critical problem.
Ultrasonography can accurately diagnose RLV and prevent unnecessary treatment [1,5-7]. We describe two cases of RLVs in a non-pregnant woman and a pregnant woman, both of which were diagnosed using ultrasonography, and review the literature.
Case Reports
Case 1
A 33-year-old non-pregnant woman, parity 2, visited our hospital with a palpable mass and pain in the left groin. Her previous pregnancies had been uneventful. Ultrasonography was performed with the 12-MHz linear array transducer of an iU22 scanner (Philips Healthcare, Bothell, WA, USA). Grayscale ultrasonography showed a mass in the left groin composed of dilated, echo-free, tubular channels. The color Doppler ultrasonography identified a mass composed of multiple echo-free tubular channels with hypervascularity that became more prominent during a Valsalva maneuver. There was no ultrasonographic evidence of a herniated bowel or lymphadenopathy (Fig. 1A, B). The patient was treated conservatively.
A 33-year-old women with round ligament varicosities.
A. Grayscale sagittal ultrasonography shows a mass in the left groin composed of multiple echo-free serpentine tubular channels. B. Color Doppler ultrasonography shows that the lesion is filled with color and the mass shows dilatation and increased flow during the Valsalva maneuver.
Case 2
A 28-year-old woman, gravidity 1 parity 0, presented at 21 weeks’ gestation with a painful swelling in the left groin. The symptoms had started 1 week earlier. On physical examination, she had a small tender soft mass in the left groin. Ultrasonography of the groin was performed using the 12-MHz linear array transducer of an iU22 scanner. Grayscale ultrasonography showed a mass in the left groin composed of multiple echo- free serpentine tubular channels. Color Doppler ultrasonography revealed hypervascularity and venous flow within the lesion (Fig. 2A, B). The patient was treated conservatively. Five weeks later, she revisited our hospital with the feeling of slightly more swelling of the left groin. Repeated ultrasonography was performed and revealed slight enlargement of multiple dilated varicose veins in the left groin, which became more prominent during the Valsalva maneuver and in an erect position. Multiple varicose pelvic veins in the left parauterine space showed continuity with the varicose veins located in the left inguinal canal (Fig. 2C-F). Neither omentum, bowel, thrombosis, nor venous rupture was identified. Conservative management was used, the patient had a normal vaginal delivery at 40 weeks. The symptoms resolved completely by three weeks postpartum.
A 28-year-old women at the 21st week of pregnancy with round ligament varicosities.
A. Grayscale transverse ultrasonography shows an ovoid multiseptated cystic mass in the left groin. B. Color Doppler ultrasonography shows that the lesion is hypervascular. After 5 weeks, follow-up ultrasonography was performed (C-F). The mass in the left groin shows slightly enlarged and composed of multiple anechoic serpentine tubular channels on grayscale ultrasonography (not shown). C. Color Doppler sagittal ultrasonography during Valsalva maneuver. The mass expands and shows marked flow augmentation. D, E. Sagittal ultrasonography of the left groin through the inguinal canal in an erect position. The lesion is enlarged and the vascularities of the mass are markedly engorged. F. These varicose veins between the markers continue to the left parauterine space (arrows) through the inguinal canal (arrowheads).
Discussion
The round ligament passes from the lateral uterus, through the internal abdominal ring, and along the inguinal canal to the labia majora. RLV arise from the veins draining the round ligament and the inguinal canal into the inferior epigastric vein [8].
RLV is more common in pregnancy, and several mechanisms contribute to varicose vein formation of the round ligament during pregnancy: progesterone-mediated venous smooth muscle relaxation causing dilatation of the round ligament veins during pregnancy, a raised cardiac output causing increased venous return and leading to engorgement of the venous tributaries, and most importantly, relative pelvic venous impingement by the gravid uterus [1,2].
RLV, like an inguinal hernia, may present with swelling and tenderness in the groin region, which can be enlarged by increased abdominal pressure in cases of coughing or the Valsalva maneuver. Both RLV and inguinal hernias can occur in the second trimester of pregnancy; therefore, RLV are easily misdiagnosed as an obstructed hernia.
The diagnosis of RLV can be established by ultrasonography [1,5-7]. The characteristic ultrasonographic findings include a prominent venous plexus with accompanying dilated draining veins and the typical "bag of worms" appearance of smaller varices on color Doppler image. The change in the shape of the cystic masses during the examination in the supine and upright positions as well as at rest and during the Valsalva maneuver are also characteristic [7,9]. The ultrasonography criteria that may be used to diagnose RLV include: multiple dilated veins passing through the inguinal canal, absence of bowel or lymph nodes in the inguinal mass, and veins seen to drain into the inferior epigastric vein [10].
The Table 1 summarizes the clinico-radiological features of the previously reported cases in the English-language literature including the present cases [1,4,9-19]. The mean age of previously reported cases of RLV was 29.7 years (range, 18 to 40 years) and site of development site was the right, followed by the left and then by both sides in the ratio of 11:9:6. All of the cases except one of ours developed during pregnancy. The symptoms were simple groin swelling in 14 cases and a painful groin mass in 12 cases. All of the cases except one were treated conservatively and subsided after delivery. In one case, surgical excision was performed for bilateral RLV during a 3rd pregnancy. In general, no specific complication was associated with RLV, except one case that presented with thrombosed varices of the round ligament.
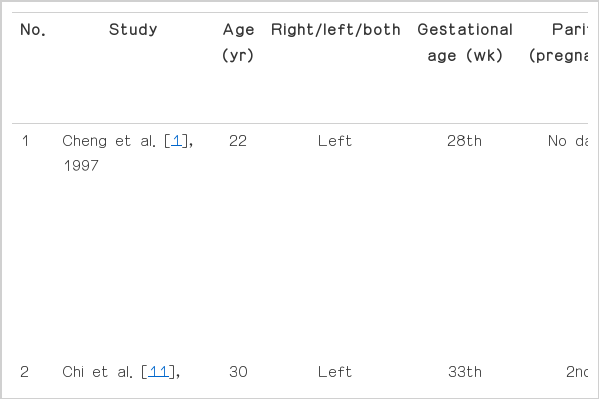
Clinico-radiologic features of 24 reported and the 2 present cases of round ligament varicosities
The differential diagnoses of RLV includes inguinal hernia, lymphadenopathy, cystic lymphangioma, endometriosis, and all cases of groin lumps presenting during pregnancy [1,9,10]. The ultrasonographic finding of indirect inguinal hernia may be characterized by the fact that the herniated contents can be seen to pass laterally to the inferior epigastric artery at its origin and the herniated bowel may have peristalsis, mucosal blood flow, or mesenteric fat [20]. Lymphadenopathy may show a hypoechoic reniform appearance with an echogenic central hilum. The ultrasonographic findings of the lymphangioma or endometrioma is nonspecific but may show a well-defined unilocular or multilocular, predominately cystic mass containing diffuse homogeneous hypoechoic material.
After a correct diagnosis of RLV, the RLV should be managed conservatively and non-surgically, mostly so it will not affect a normal vaginal delivery. However, RLV requires close monitoring during pregnancy as rupture and thrombosis of the RLV may occur and result in an intense painful swelling in the groin [21]. Upon imaging, if the veins are non-compressible, no flow signal can be obtained, and/or there is a visible clot within the lumen, complicated RLV should be suspected and emergency surgical exploration is recommended [10,21].
RLV should be considered a part of the differential diagnosis of an inguinal mass of women, especially during pregnancy, and ultrasonography can accurately diagnose RLV. By becoming familiar with the ultrasonographic findings of RLV, RLV can be treated optimally, and unnecessary surgical intervention and associated morbidity can be prevented.
Notes
No potential conflict of interest relevant to this article was reported