

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
The widespread use of high-resolution neck ultrasonography (US) for thyroid lesions has increased the frequency of incidentally detected parathyroid lesions [1,2]. An incidentally discovered parathyroid lesion on neck imaging for a non-parathyroid disease is called a parathyroid incidentaloma [1,3]. Parathyroid lesions are suspected when extrathyroid soft tissue is seen at the posterior and inferior portions of the thyroid gland, separated from the thyroid parenchyma. However, in such cases, a parathyroid lesion should be differentiated from exophytic thyroid nodule, lymph node (LN), normal fat, and other soft tissue mass. It is often difficult to differentiate parathyroid lesions from non-parathyroid lesions owing to overlapping imaging findings [4,5]. Therefore, fine-needle aspiration (FNA) is needed to distinguish parathyroid lesions from non-parathyroid lesions. Several studies have reported the diagnostic performance of FNA cytology (FNAC) and washout parathyroid hormone (PTH) measurements for the diagnosis of parathyroid adenoma [1,3,6-13]. However, limited studies have evaluated the diagnostic performance of FNAC for parathyroid incidentaloma [3]. Therefore, this study aimed to evaluate the diagnostic role of FNAC and analyze the factors associated with false-negative results of FNAC in patients with parathyroid incidentaloma who were referred for US-guided FNA of thyroid nodules.
Materials and Methods
Compliance with Ethical Standards
This retrospective study was approved by the review board of the authors’ affiliated institution (Asan Medical Center 2021-1861), and written informed consent was obtained from all patients before performing FNA.
Patient Selection
Consecutive patients who underwent US-guided FNAC with measurements of washout PTH at the authors’ institution between January 2015 and May 2020 were included. Patients were included if they underwent US-guided FNA with measurement of washout PTH for an incidentally detected suspected parathyroid lesion. Patients were excluded if (1) they underwent US-guided FNA with measurement of washout PTH for the evaluation of hypercalcemia or hyperparathyroidism, (2) had a known history of parathyroid lesions, or (3) if the evaluated lesion was identified as a pure cyst. Finally, 121 suspected parathyroid lesions from 121 patients were included in this study.
US-Guided FNA and FNA-PTH
Ultrasound examination of the thyroid was performed using an iU22 or HDI-5000 unit (Philips Healthcare, Bothell, WA, USA) or an EUB-7500 unit (Hitachi Medical Systems, Tokyo, Japan) with a 5-14-MHz linear high-frequency probe. All US examinations and US-guided FNA procedures were performed by radiologists under the supervision of staff radiologists having more than 14 years of experience in thyroid imaging. Before performing FNA, thyroid and neck US examinations were performed. When a well-defined, oval, hypoechoic or isoechoic nodule was noted as being separate from the thyroid parenchyma, parathyroid incidentalomas were suspected [1]. When parathyroid incidentalomas were suspected, PTH measurements from the washout fluid were performed in addition to FNAC.
FNA was performed under US guidance with a free-hand technique using a 23-gauge needle connected to a 10-mL syringe. All FNA specimens were prepared from liquid-based cytology. The specimens were prepared using a ThinPrep 2000 processor (Hologic Co., Marlborough, MA, USA). The same needle and syringe were rinsed with 1 mL of normal saline, and PTH was measured in the washout fluid. If there was more than 1 mL of aspirate, PTH was measured in this fluid without adding saline. The cytology findings were interpreted by cytopathologists specializing in thyroid and parathyroid cytology. PTH assays were performed using commercial polyclonal antibody immunoradiometric assay kits.
Image Analysis
US images were reviewed retrospectively and independently by two radiologists with 11 and 10 years of experience, respectively, in thyroid US. Neither reviewer had any knowledge of the patients’ clinical histories, previous imaging results, or cytopathology results. Any discrepancy between the two reviewers was resolved by consensus. US findings of the nodules were evaluated for the following features: the nodule’s size, depth, and location; the presence of normal thyroid tissue along the course of needle insertion; echogenicity (hyperechoic, isoechoic, or hypoechoic); the presence of cystic change; and intranodular vascularity.
Biochemical and Scintigraphy Study
In patients with parathyroid lesion, biochemical studies including serum PTH and total calcium levels and scintigraphy were performed.
Reference Standard
The final diagnosis of a parathyroid lesion was made upon: (1) confirmation of a surgical specimen or (2) a washout PTH measurement higher than 65 pg/mL-the upper normal limit of PTH in a blood test. Lesions deemed free of parathyroid lesions by the same criteria were finally diagnosed as non-parathyroid lesions.
Statistical Analysis
Continuous variables are expressed as mean±standard deviation, and categorical variables are shown as percentages. To evaluate differences in patients’ demographic data between lesions of parathyroid and non-parathyroid origin, the Student t-test was used for continuous variables, while the chi-square test or Fisher exact test was used for categorical variables.
The cytologic results were classified as parathyroid or non-parathyroid based on their origin. The diagnostic performance of FNAC for parathyroid lesions was assessed using sensitivity, specificity, the positive predictive value (PPV), the negative predictive value (NPV), and diagnostic accuracy.
To evaluate differences in clinicoradiologic features between true-positive and false-negative results on the FNAC of parathyroid lesions, the chi-square test or Fisher exact test was used for categorical variables, while the Student t-test was used for continuous variables. The statistical analysis was performed using SPSS version 23 (IBM Corp., Armonk, NY, USA).
Results
Study Population
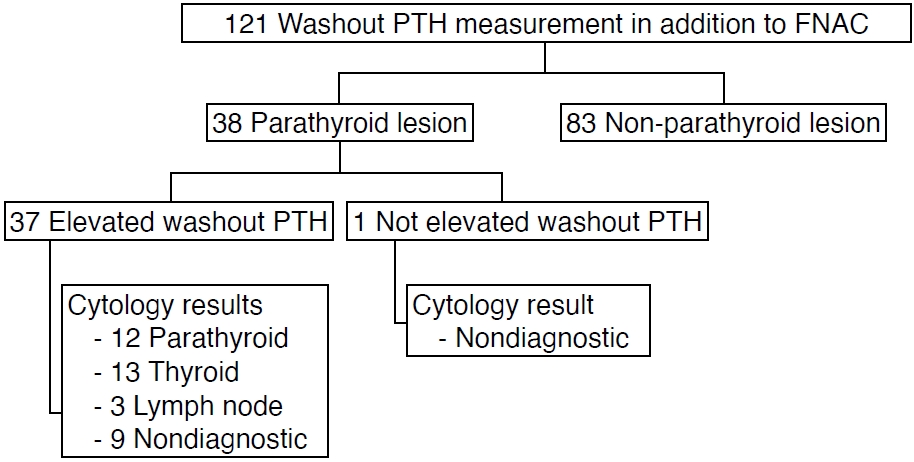
A total of 121 patients underwent FNAC and washout PTH measurements for 121 suspected parathyroid lesions. Of these lesions, 38 were parathyroid lesions (31.4%), and 83 were nonparathyroid lesions (68.6%). The diagnosis of parathyroid lesions was based on surgical confirmation in 21 patients and elevated washout PTH in 17 patients (Fig. 1). The pathologic results of the surgical specimens were parathyroid adenoma (n=20) and atypical parathyroid adenoma (n=1). All parathyroid lesions showed elevated washout PTH, except for one case, which showed a washout PTH level of 8.9 pg/mL; the FNAC result was nondiagnostic, and the lesion was confirmed as a parathyroid adenoma after surgery. A retrospective image review indicated that this discrepancy was attributable to mistargeting of the nodule. Serum PTH was measured in 34 patients with parathyroid lesions. The serum PTH level was elevated in 26 patients (67.9-671 pg/mL) and normal in eight patients (39.1-63.6 pg/mL). The serum ionized calcium level was elevated in 22 patients (10.2 to 12.3 mg/dL) and non-elevated in 14 patients. Among 83 patients with non-parathyroid lesions, 71 (85.5%) had specific cytologic results, as follows: thyroid lesion (n=59), LN (n=11), and neurogenic tumor (n=1). The remaining 12 patients (14.5%) showed nondiagnostic results on FNAC, and the lesions were identified as comprising fat tissue, LN, and thyroid tissue on follow-up. There were no complications after FNA.
Scintigraphy was performed in 26 of 121 patients, including 20 patients with parathyroid lesions and six patients with non-parathyroid lesions. Of the six patients with non-parathyroid lesions, two patients had false-positive results on scintigraphy, and all 20 patients with parathyroid lesions revealed sestamibi uptake. Therefore, the sensitivity and specificity of scintigraphy were 100% and 66.7%, respectively. The lesions showing false-positive scintigraphy results in two patients were confirmed as thyroid nodules.
Table 1 shows the differences in the clinical and radiologic features between parathyroid and non-parathyroid lesions. Parathyroid lesions more commonly showed hypoechogenicity than non-parathyroid lesions (94.7% vs. 60.2%, P<0.001) and intranodular vascularity (92.1% vs. 59.0%, P<0.001). There was no difference in the mean age of the patients, size of the lesion, or the proportion of cystic change between the two groups.
Diagnostic Performance of FNAC
Table 2 shows the diagnostic performance of FNAC for the diagnosis of parathyroid lesions. The sensitivity, specificity, PPV, NPV, and diagnostic accuracy of FNAC for the diagnosis of parathyroid lesions were 31.6% (12/38), 100% (83/83), 100% (12/12), 76.1% (83/109), and 78.5% (95/121), respectively. There were 26 false-negative results on FNAC (68.4 %). The most common results were thyroid lesion (atypia of undetermined significance [n=8] and benign follicular nodule [n=5]), followed by nondiagnostic results (n=10), and LN (n=3).
Factors Associated with False-Negative Results on FNAC
Table 3 shows a comparison of the clinical and radiologic features of cases with false-negative and true-positive results on FNAC for the diagnosis of parathyroid lesions. The number of false-negative and true-positive results in FNA cases differed significantly. The proportion of cases where FNA was performed twice was significantly higher in the true-positive cases than in the false-negative cases (58.3% vs. 23.1%, P=0.043). Other clinicoradiologic features, including size, distance from the nodule, location, overlying thyroid gland, cystic change, vascularity, echogenicity, and proficiency of the operator, showed no differences between the two groups.
Discussion
In the present study, 68.6% of patients who underwent FNA for parathyroid incidentaloma were diagnosed with non-parathyroid lesions. The diagnostic performance of FNAC for parathyroid incidentaloma showed a low sensitivity of 31.6%. A meaningful correlation was found between performing FNA twice and true-positive results of FNAC for parathyroid lesions. Therefore, when FNA is performed for parathyroid incidentaloma, as the sensitivity of FNAC for diagnosing parathyroid lesion is low, washout PTH measurements should be added. In addition, performing FNAC twice can improve the accuracy of FNAC for the diagnosis of parathyroid lesions, as well as many diseases that can mimic parathyroid lesions.
Parathyroid incidentaloma on thyroid US was more common than expected, as the prevalence of suspected parathyroid lesions was reported to be 0.45%-0.6% [1,3]. Parathyroid lesions can be suspected when extra thyroid soft tissue is seen at the posterior portion of the thyroid gland, separate from the thyroid parenchyma. However, in this situation, parathyroid lesions should be differentiated from exophytic thyroid nodules, LNs, normal fat, and other soft tissue masses. In this study, the most common final diagnosis of suspected parathyroid lesions on thyroid US was exophytic thyroid nodule (n=67, 55.4%), followed by parathyroid adenoma (n=38, 31.4%), LN (n=13, 10.7%), fat (n=2, 1.7%), and neurogenic tumor (n=1, 0.8%). In this study, hypoechogenicity of the nodule and intranodular vascularity were more often seen in parathyroid lesions than in non-parathyroid lesions (P<0.001). These results are consistent with previous studies [14-20]. The intranodular vascularity of parathyroid adenomas is related to the polar feeding vessel arising from the inferior thyroidal artery branches [17], and hypoechogenicity results from the high cellularity of parathyroid adenomas (with chief cell proliferation) and their low content of fatty tissue [18-20].
Because US examinations are performed to localize the lesions when evaluating patients with hyperparathyroidism, FNA is not essential. Furthermore, FNA for parathyroid adenomas has potential risks, including tumor seeding, massive hemorrhage, parathyromatosis, recurrence, or histological alterations following FNA [21-27]. However, for parathyroid incidentalomas, FNA is often needed to differentiate various diseases that can overlap with parathyroid lesions [28]. The diagnostic ability of FNAC to distinguish parathyroid lesions from thyroid lesions is known to be limited [1,3,7-13]. Previous studies have reported that the diagnostic sensitivity of FNAC in the diagnosis of parathyroid lesions was 29%-41.7% [3,7,8]. However, several other studies have reported a relatively high sensitivity of FNAC for the diagnosis of parathyroid lesions (86%–86.7%), and the available clinical information, such as high serum PTH, may explain these differences [29,30]. In the present study, which analyzed the diagnostic performance of FNAC for parathyroid incidentaloma without clinical information, including hyperparathyroidism, the sensitivity was low (31.6%). Of the cytologic results of 26 false-negative cases in FNAC, the most common results were thyroid lesion (n=13, benign or follicular lesion of undetermined significance), followed by nondiagnostic results (n=10) and LN (n=3). Based on FNAC, parathyroid lesions are commonly misdiagnosed as Hürthle cell thyroid neoplasms [31-34] or chronic lymphocytic thyroiditis [14] owing to similarities in cellular morphology, including the presence of follicular and papillary structures, colloid-like material, macrophages and paravacuolar granules [31,35-38]. The presence of oncocytic cells or naked nuclei in parathyroid lesions may be confused with Hürthle cell thyroid neoplasm and lymphocytes, respectively [6,38]. This is the reason why washout PTH measurements are recommended to assess and incidentally detect suspected parathyroid lesions in the neck. For nodules without elevated washout PTH levels, in 84.5% (71/84) of cases, specific cytologic results could be obtained using FNAC. FNAC for the evaluation of parathyroid incidentaloma plays a more important role in the diagnosis when the lesion is not a parathyroid lesion. Therefore, it is important to measure washout PTH combined with FNAC when performing FNA for parathyroid incidentaloma to properly manage these patients.
Sestamibi scintigraphy is widely used to localize parathyroid adenomas, especially in preoperative evaluations of patients with primary hyperparathyroidism. One meta-analysis reported that sestamibi scintigraphy had a higher sensitivity than US (88% vs. 78% for single adenomas) [39]. In addition, combined US and scintigraphy had higher sensitivity, specificity, and accuracy [40-42]. In the present study, the sensitivity of scintigraphy was 100%. Considering the high sensitivity of scintigraphy, it can be used as a complementary method for reducing the false-negative results of FNA of parathyroid incidentaloma. However, false-positive results on scintigraphs should also be considered. Solitary thyroid adenoma or multinodular goiter, LN, or metastasis may have false-positive findings on scintigraphy [43-47]. In this study, two patients with thyroid nodules showed false-positive results on scintigraphy.
The clinical and radiologic factors associated with false-negative results of FNAC were analyzed. US features, such as size, echogenicity, cystic change, vascularity, the location and depth of nodules, and the operator’s proficiency, did not reach statistical significance, whereas the number of FNAs was significantly associated with false-negative results on FNAC. The cases of elevated washout PTH despite nondiagnostic cytology may indicate that it is difficult to make an accurate diagnosis due to an insufficient number of cells [48]. Therefore, performing FNA twice or more in parathyroid incidentaloma can improve the accuracy of FNAC for the diagnosis of parathyroid lesions, as well as many diseases that can mimic parathyroid lesions.
This study has several limitations. One of the limitations is its retrospective design. All patients were recruited at a single tertiary referral center, leading to unavoidable selection bias. The final diagnosis of the majority of non-parathyroid lesions (89.2%) was based on FNA results and follow-up imaging studies. This may have caused false-negative results. In addition, the retrospective assessment of static US images has an inherent limitation to the accuracy of US interpretation. Thus, further large-scale, prospective, and multicenter studies are required to validate these results.
In conclusion, considering the low sensitivity of FNAC, the use of washout PTH in addition to FNAC is necessary to accurately diagnose parathyroid incidentaloma on thyroid US. In addition, performing FNAC twice can improve the accuracy of FNAC for the diagnosis of parathyroid lesions, as well as many diseases that can mimic parathyroid lesions.
 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI



