

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
Globally, approximately 2 million patients have been diagnosed with end-stage renal disease (ESRD), with an annual reported incidence of nearly 100,000 cases [1]. Patients with ESRD require some form of renal replacement therapy, with hemodialysis typically being the preferred treatment. Hemodialysis is commonly performed by placing two large-bore needles into a vascular access point in the upper extremity. Simply put, blood is drawn into the dialysis machine through one needle access, cleaned, and then returned to the patient through the second needle access [2].
Long-term hemodialysis typically necessitates vascular access in the upper extremity, either through an arteriovenous fistula (AVF) or an arteriovenous graft (AVG). Central venous catheters can also provide vascular access for patients undergoing hemodialysis, but these devices are associated with a substantial risk of infection, which increases morbidity and mortality. Regardless of the type of vascular access used, it is necessary to conduct surveillance through physical examination and imaging to identify potential complications and access failure. Ultrasonography (US) is a valuable tool for preoperative evaluation of the arterial and venous vasculature in the upper extremity [1]. This manuscript discusses the importance of multiparametric US in evaluating AVF and AVG.
AVF and AVG
AVFs are the preferred method for hemodialysis vascular access, compared to AVGs and central venous catheters. This is due to the lower risk of thrombosis and infection associated with AVFs, as well as their longer patency duration [1]. An AVF is surgically created by connecting a native vein and artery using an end-to-end, end-to-side (vein-to-artery), or side-to-side anastomosis. This is typically done on the non-dominant wrist or upper arm, provided the vascular anatomy on that side is suitable (Fig. 1). However, AVFs have some disadvantages, including a longer time to maturation (4-6 weeks) compared to AVGs and a higher risk of maturation failure. The most common types of AVFs are radiocephalic and brachiocephalic fistulas. The brachial artery and basilic vein can also be used, but creating this type of AVF requires a second transposition procedure [1].
An AVG is a prosthetic conduit consisting of polytetrafluoroethylene or a bovine carotid artery graft, placed under the skin to establish a communication between an artery and a vein. AVGs require a shorter maturation period than AVFs (2-4 weeks) and can be utilized with smaller-caliber veins. This makes them a suitable choice for patients with limited venous access options. However, AVGs carry a higher risk of thrombosis and infectious complications compared to AVFs [1].
Central venous catheters serve as a temporary solution for vascular access. However, due to the high risk of infection associated with these catheters, it is advisable to replace them promptly with an upper-extremity AVG or AVF [3].
Preoperative Mapping with US
Prior to fistula creation, a proper assessment of the arterial and venous system should be conducted. This evaluation should include a physical examination and color Doppler US, as well as computed tomography, magnetic resonance imaging, or digital subtraction angiography, as clinically warranted. In combination with the patient’s history and physical exam, these examinations should allow clinicians to perform an adequate evaluation of the anatomical and functional features of the vasculature to determine which patients are suitable candidates for surgical AVF or AVG creation [1,4].
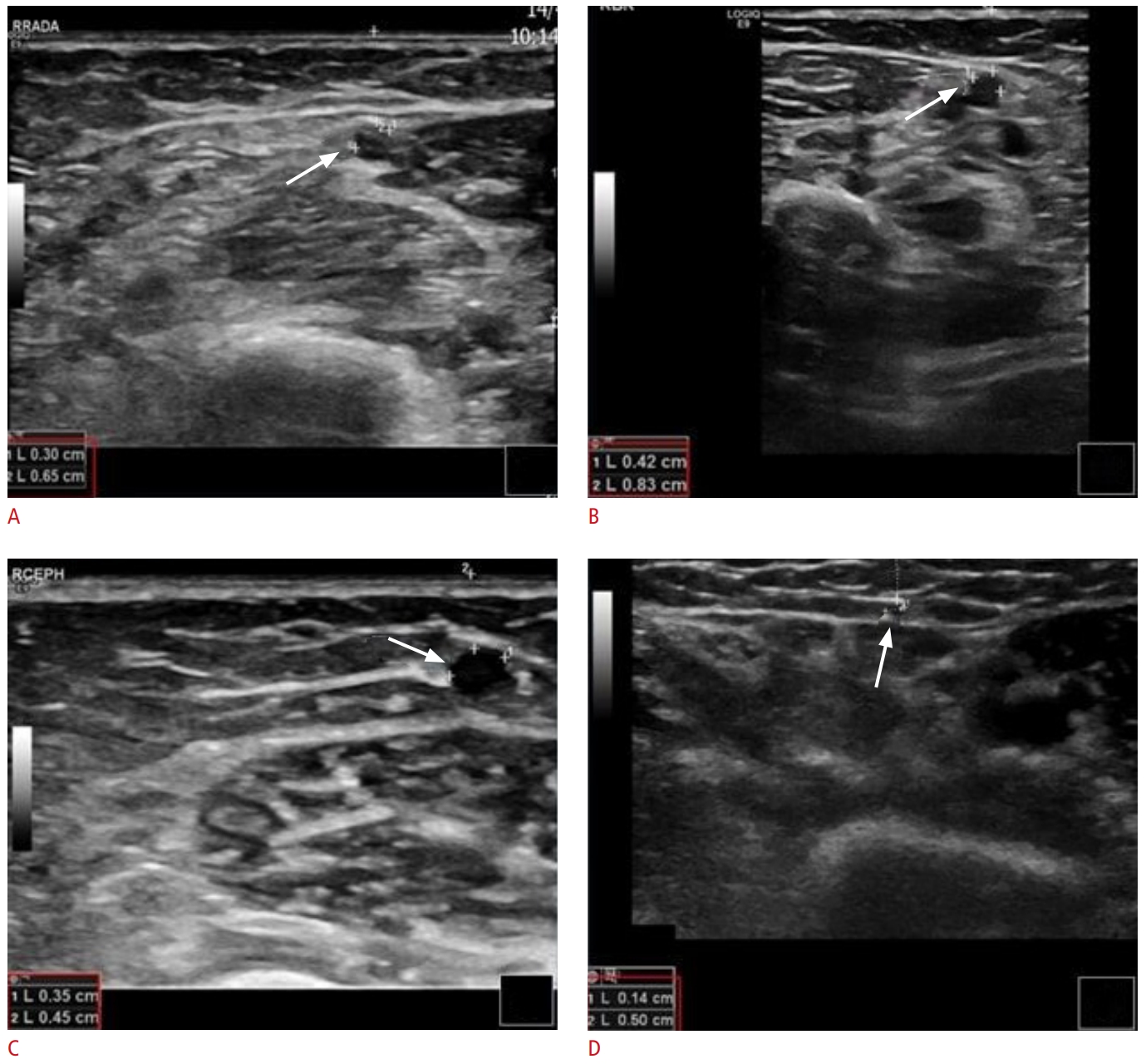
High-frequency linear transducers (>7.5 Hz) should be utilized for the US examination. The examination room should be warm, and a substantial amount of body-temperature gel should be applied to prevent vasospasm [1,5]. Initially, grayscale, color Doppler, and pulsed-wave Doppler imaging should be used to examine the arteries and veins of the non-dominant arm. If no suitable vessels for fistula formation are found, the dominant arm should then be examined [6]. The arterial examination should include the subclavian, axillary, brachial, radial, and ulnar arteries. Each artery should be evaluated for its patency, course, and any presence of obstructive atherosclerotic disease. The depth of the artery from the skin should also be measured (Fig. 2). The internal diameter of the artery intended for fistula creation should be at least 2 mm. Functional characteristics of the arteries should be assessed using spectral Doppler imaging, including the evaluation of blood flow and the capacity of the vessel to dilate. Blood flow can be determined by calculating the vessel’s diameter and the mean peak systolic velocity (PSV) (cm/s) in the longitudinal plane. Previous studies have shown that a radial artery flow volume greater than 50 mL/min is associated with successful radiocephalic AVF formation. Conversely, a preoperative radial artery flow volume of less than 20 mL/min is linked to an increased risk of AVF failure within the first 8 months. The capacity of arteries to dilate can be estimated using the reactive hyperemia test [1,5].
Preoperative venous mapping encompasses the examination of both superficial and deep venous systems, extending from the wrist to the visible central veins. It is crucial to assess all veins for patency through compression, as they will be noncompressible if they are partially or fully thrombosed. The vein lumen is scrutinized for any echogenic material representing thrombus or stenoses. The thickness of the wall and the diameter of the vessel are also evaluated. For AVF creation, it is recommended that the venous diameter be at least 2.5 mm with a tourniquet and 2 mm without one. The course of the veins is mapped, and ideally, a vein used for outflow should have a reasonably linear path. Another important parameter to examine is the depth of the vein from the skin, which should be less than 5 to 6 mm for a length of 10 cm or more to ensure successful needle cannulation [1,5]. The visualization of central veins using US is limited. Therefore, the proximal segments of the subclavian vein, innominate vein, and superior vena cava are best assessed with digital subtraction venography. This technique employs either iodine-based contrast or carbon dioxide as a contrast agent, depending on the clinical situation [1,5].
Normal US Findings of Upper Extremity Vascular Access Surveillance
Ideally, US examinations of AVFs and AVGs should be conducted more than 24 hours after the last dialysis session [7]. In these US examinations, the blood flow volume is calculated within the graft for patients with AVGs and within the brachial artery for patients with native AVFs, regardless of the subtype [7]. For a precise blood flow calculation, three consecutive measurements are recommended, except in patients with arrhythmia, where five measurements are beneficial to account for potential variability in cardiac output [8]. Most published studies suggest that an extracorporeal circuit/blood flow greater than 500 mL/min, coupled with a diameter larger than 4 mm in the venous outflow tract, represent unremarkable findings in patients with AVFs [9].
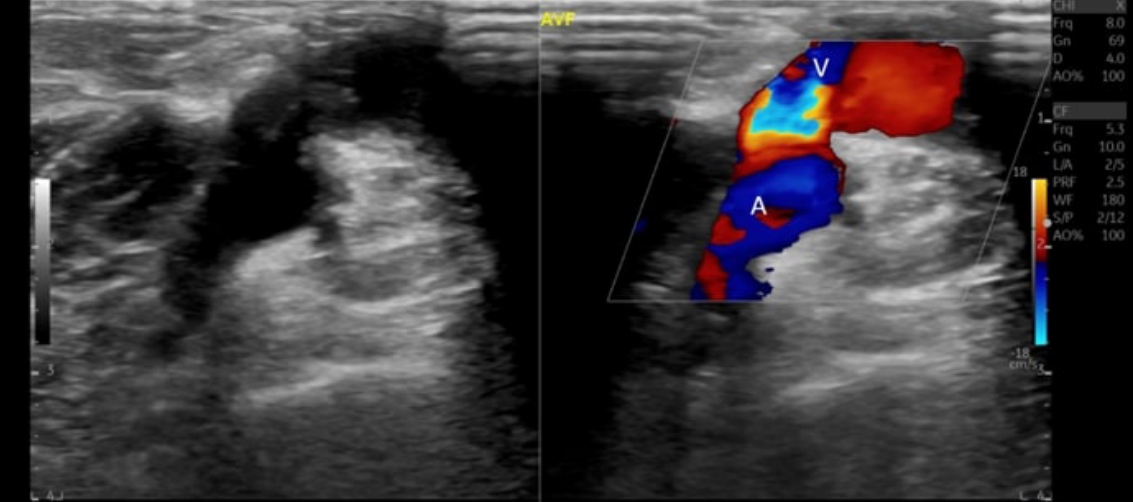
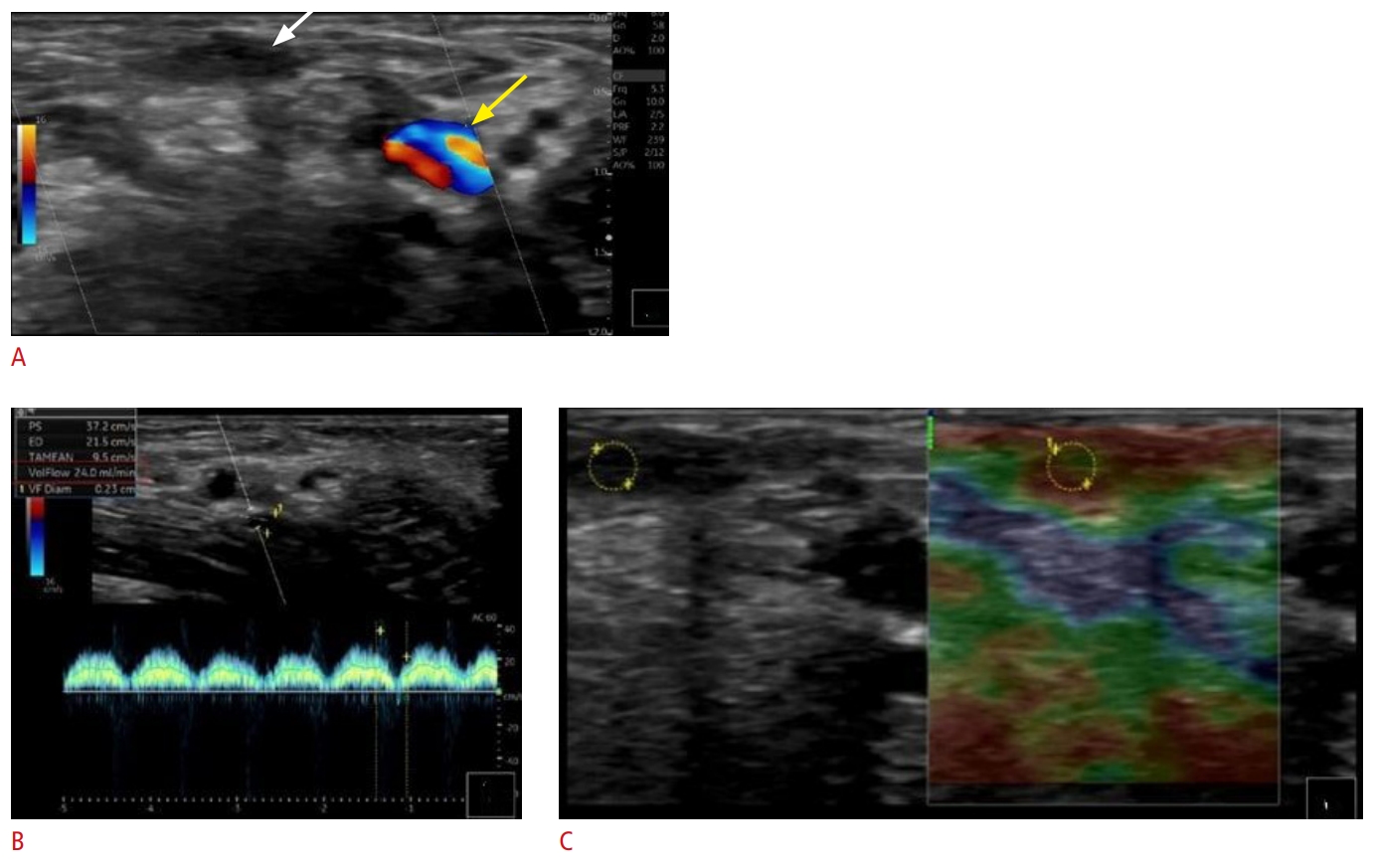
During US examinations, it is important to note any collateral vasculature near the access site. This can increase the risk of recirculation phenomena (Fig. 3) as well as extraluminal pathologies such as hematoma and subcutaneous edema [10]. Finally, to achieve successful cannulation, the tips of the two large-gauge needles must be placed at a specific distance apart to prevent recirculation phenomena. Consequently, a straight venous segment of at least 4 cm in the cannulation zone is necessary for appropriate two-needle access [7].
US Assessment of Fistula Maturation
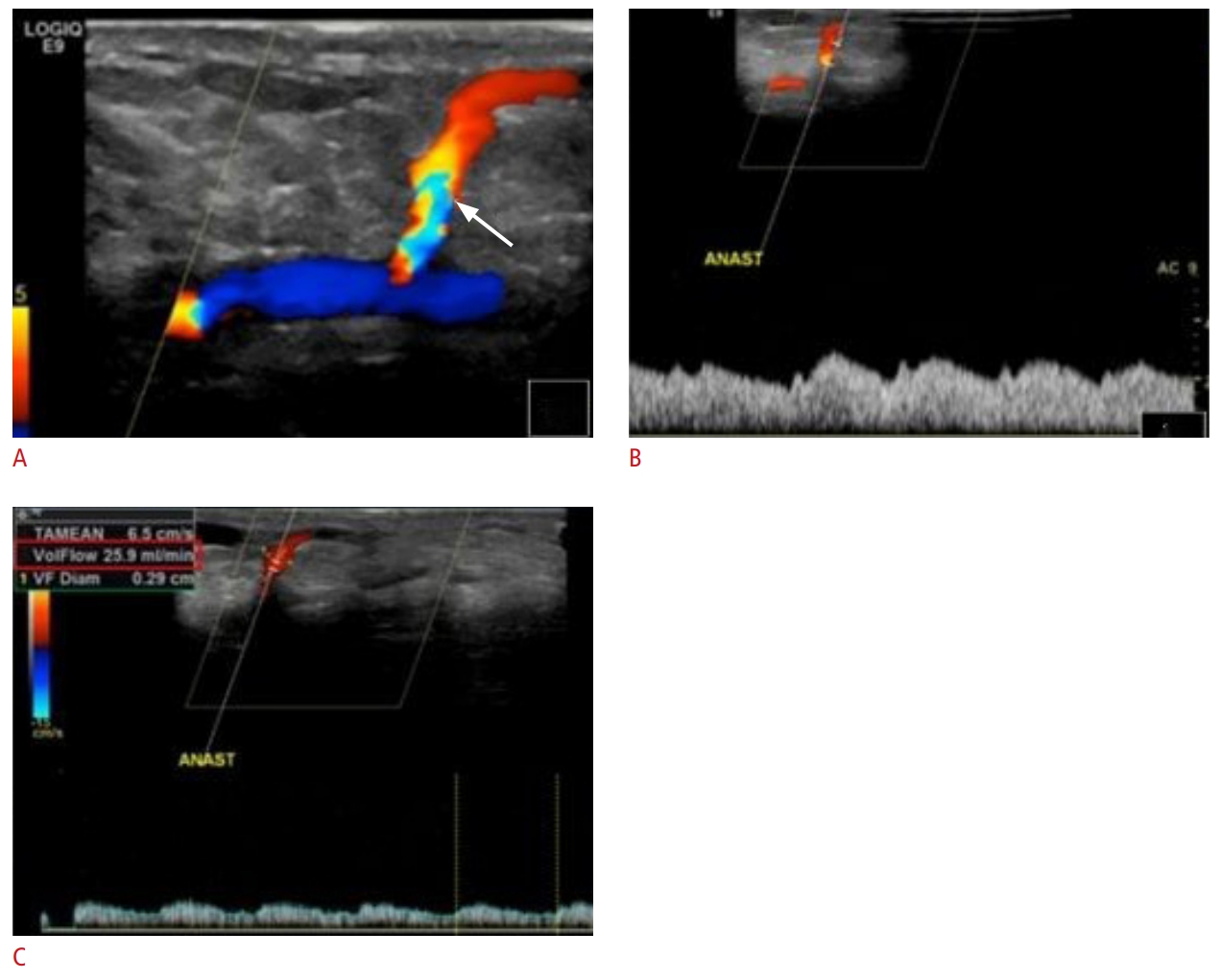
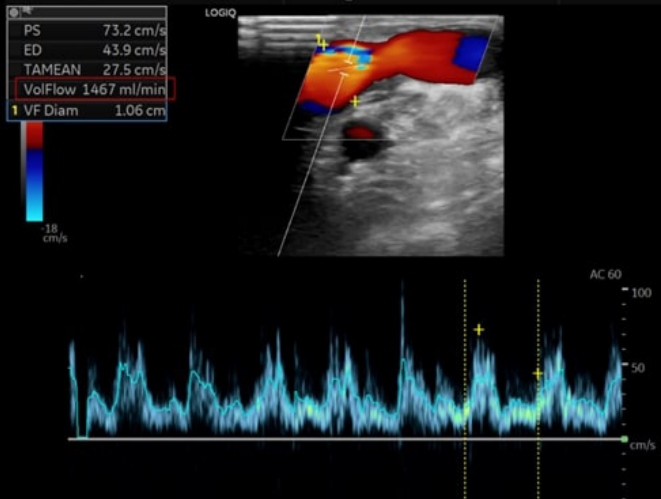
Although AVFs are the preferred method for dialysis access, they are unsuitable for proper use in approximately 20% to 60% of cases due to inadequate maturation (Fig. 4) [11,12]. Maturation is the process through which a fistula develops the necessary characteristics for successful two-needle cannulation and subsequent high-quality hemodialysis. The "rule of 6’s" (Table 1) is a commonly used guideline for this process: a mature fistula should have a diameter of at least 6 mm and clear margins during tourniquet placement within 6 weeks of surgical creation. Additionally, the access vessel depth should be less than 6 mm, and blood flow should exceed 600 mL/min (Fig. 5) [13]. Recent studies have also associated maturation with suitable hemodynamics, characterized by brisk forward flow and the absence of large venous collateral branches that could divert flow from the upper extremity vascular access [14]. In this context, vascular remodeling refers to the gradual increase in diameter and blood flow, which in turn increases the capacity of the accessed vein and venous outflow system [15]. However, one potential limitation of US maturation assessment is the lack of a clearly defined optimal location for blood flow measurements [16].
Clinical maturation refers to the capacity of a fistula to be used for hemodialysis with two large-gauge needles for at least 75% of a patient’s dialysis sessions over a 2-week period [17]. Previous studies have demonstrated that clinical maturation can be accurately predicted by palpation of a thrill in the cannulation zone during physical examination in 72% to 80% of patients [18]. However, physical examination is less effective in predicting clinical maturation in patients with thicker subcutaneous fat and in those with AVFs exhibiting delayed maturation [19]. These patients may benefit from serial US examinations to precisely monitor the maturation process.
Most AVF maturation failures can be attributed to underlying venous outflow stenosis. This condition gradually reduces blood flow in the outflow vein, which in turn alters the AVF pressure, leading to a failure to mature and eventually resulting in complete occlusive thrombosis of the upper-extremity access [20]. In a single-institution retrospective review, duplex US was found to offer better sensitivity than physical examination in identifying immature AVFs, thereby highlighting the potential need for reintervention [21]. In a separate study, the assessment of fistula maturation using Doppler US was found to correlate well with clinically significant stenosis observed on invasive fistulograms, which were used as a reference standard [22]. This study also found that most de novo stenoses in the maturation process appeared immediately after the arterialization of the superficial veins. These stenoses were primarily due to intimal hyperplasia, and Doppler US was effective in identifying them [23]. Previous studies have recommended conducting Doppler US examinations at 1, 2, and 6 weeks after surgical creation of the AVF/AVG, particularly if problems are detected during physical examinations at outpatient visits [22,23].
US Assessment of Vascular Access Complications
The necessity of maintaining functioning vascular access and managing any related complications are the primary sources of morbidity in patients with ESRD [24]. AVFs are associated with lower complication rates than AVGs and central venous dialysis catheters. The most common complications of AVFs include thrombosis, steal syndrome, aneurysm/pseudoaneurysm/hematoma formation, infection, ischemic neuropathy, exacerbation of congestive heart failure, stenosis, and lymphedema [25]. Early diagnosis and proper treatment of these conditions may improve outcomes among patients with ESRD [26].
Thrombosis
Thrombosis is a common late fistula complication that must be treated endovascularly to prevent vascular access abandonment. AVFs are associated with lower rates of thrombotic events than AVGs and central venous catheters [27]. The most common pathophysiological cause of fistula thrombosis is venous neointimal proliferation [28].
Patients with recurrent thrombotic episodes may need to be evaluated for an underlying hypercoagulable state. This could potentially be caused by homozygosity or heterozygosity for factor V Leiden, ATIII levels that are less than 60% of normal values, or a deficiency in proteins C and S. Chronic kidney disease can also lead to coagulation abnormalities, such as elevated levels of factor VIII, fibrinogen, D-dimer, and homocysteine. It may also cause a reduction in thrombin clotting time and/or the presence of antiphospholipid antibodies. Venous outflow stenosis, which can lead to stasis in the access, can also predispose patients to thrombosis in upper extremity vascular access [29,30].
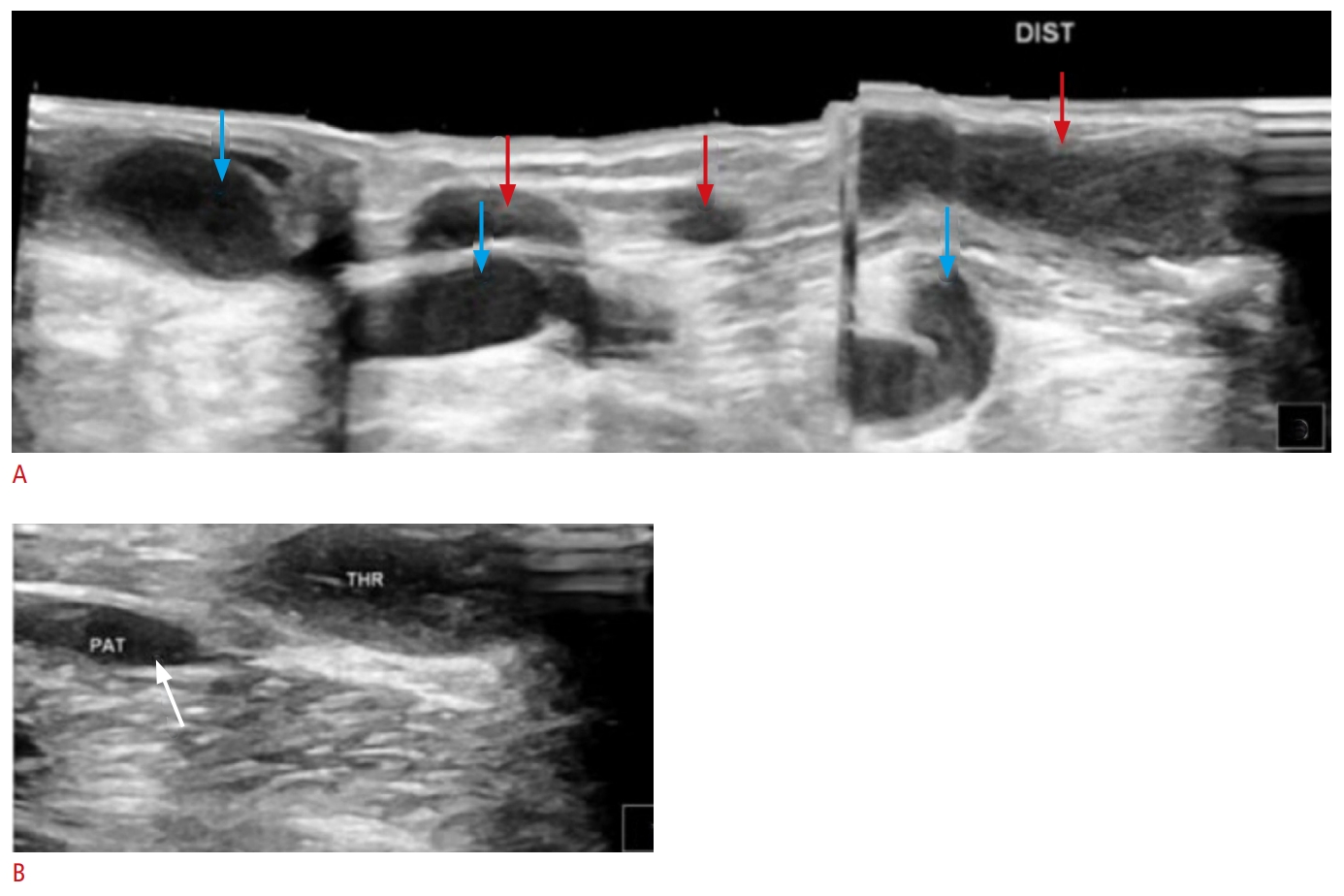
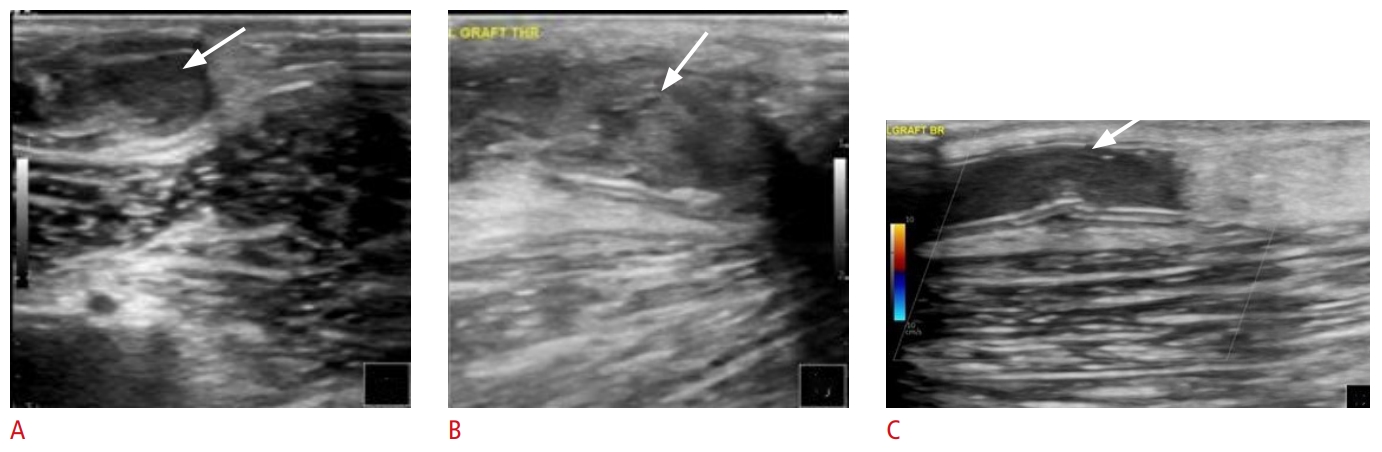
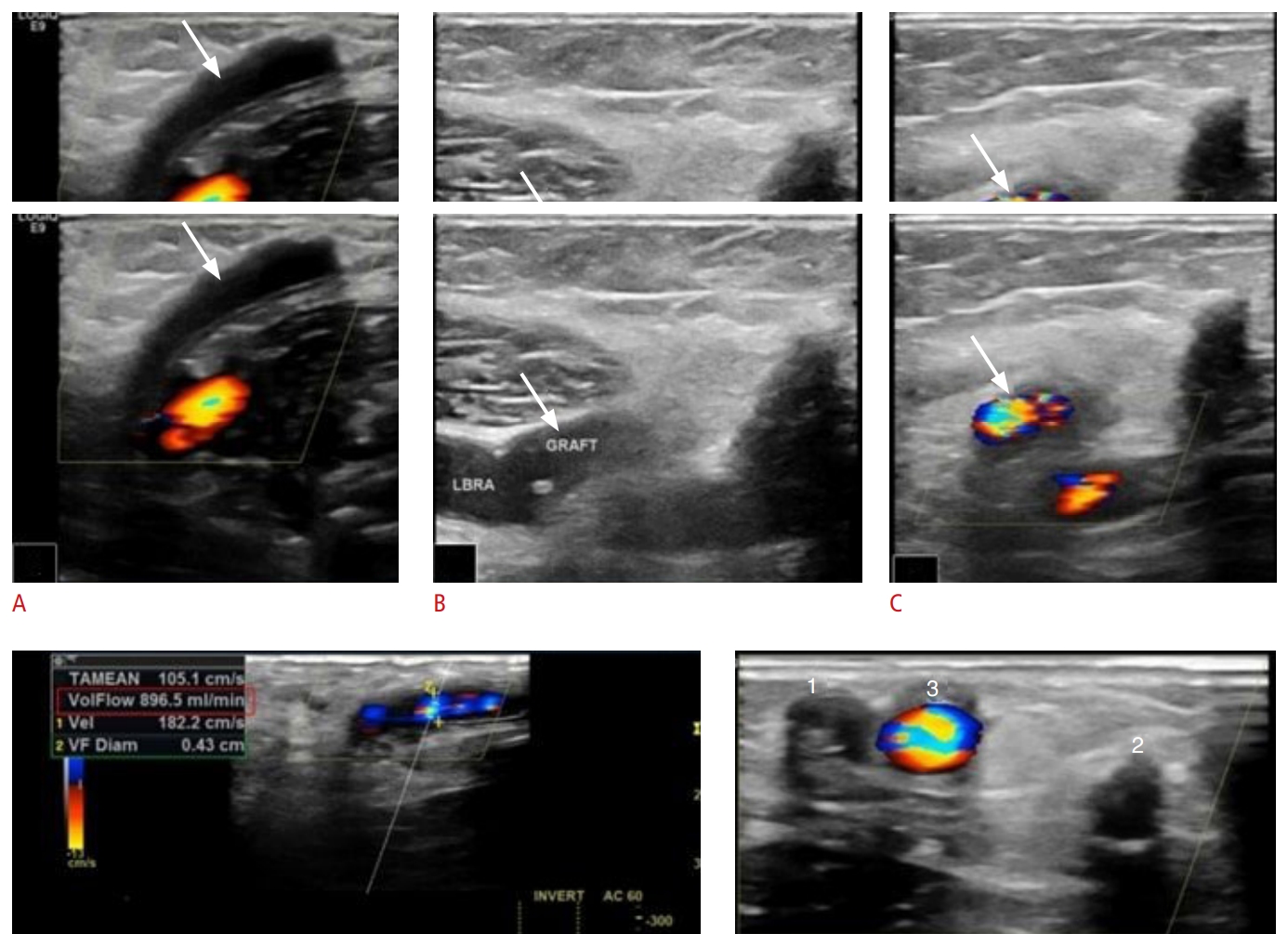
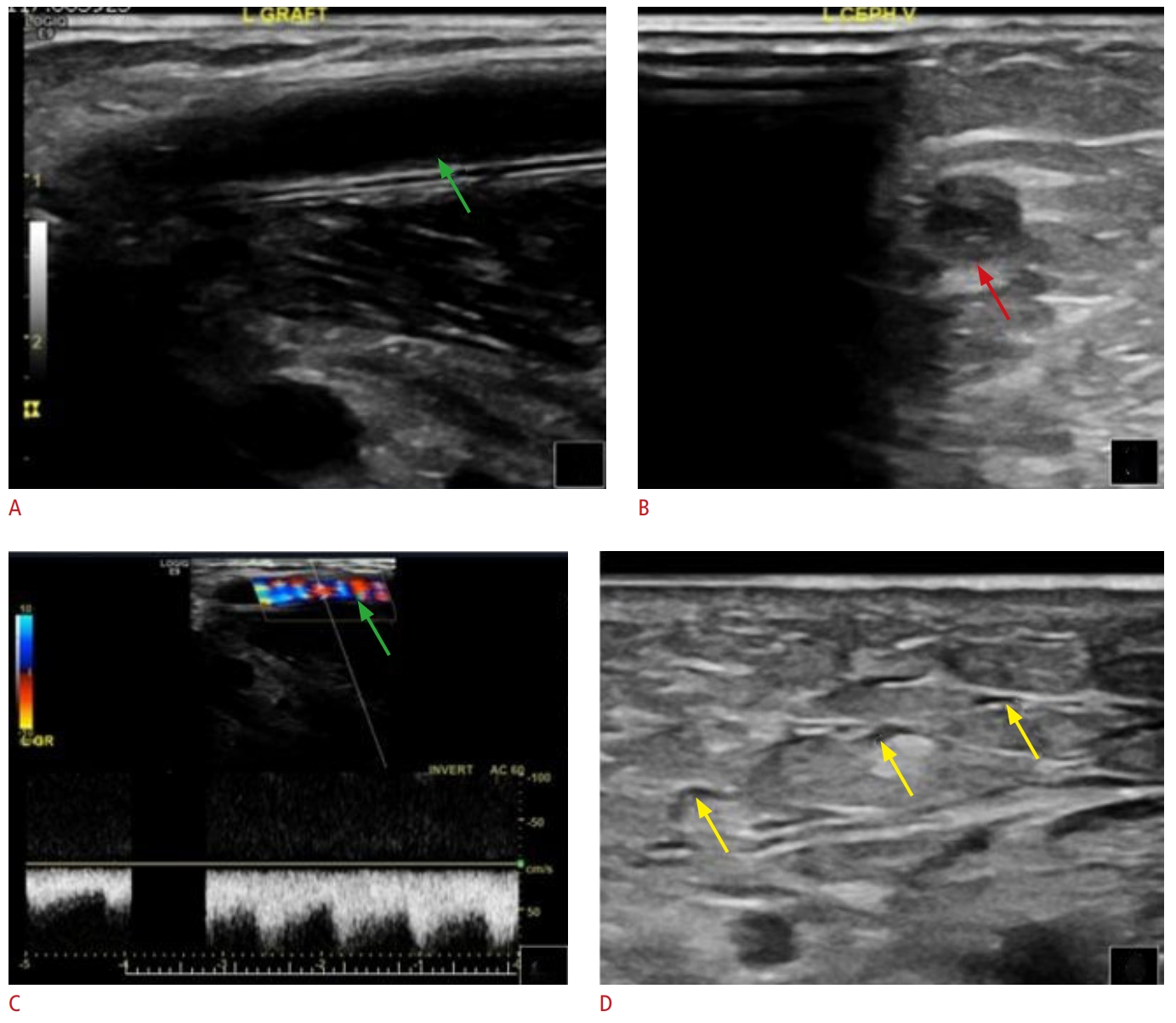
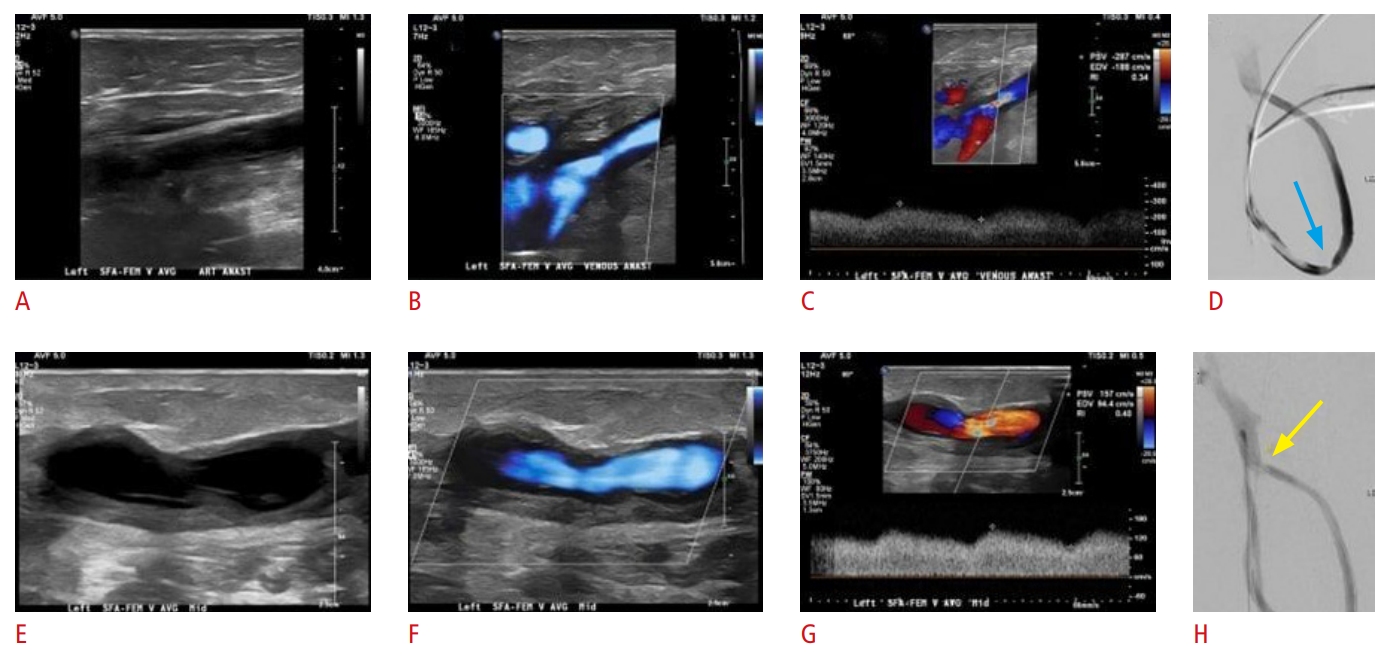
Color Doppler US is the preferred noninvasive method for diagnosing thrombosis. Typically, a clotted vein appears filled with a solid material of mixed echogenicity, is noncompressible, and does not react to dynamic tests such as the Valsalva maneuver. In the early stages, the thrombus echogenicity is low, but it increases over time as the thrombus becomes more chronic. Color Doppler US often reveals a lack of flow signals, and a persistent high-resistance triphasic trace is frequently observed within the artery that supplies the fistula (Figs. 6, 7) [29]. The thrombus may be either completely or partially occlusive (Fig. 8). Patients with acute thrombosis in AVFs usually experience sudden pain in the affected upper extremity [25]. Acute thrombosis requires immediate pharmacomechanical thrombectomy to prevent its progression into chronic thrombotic disease, which could result in permanent loss of vascular access in the upper extremity (Fig. 9). On color Doppler US, a chronic thrombus appears hyperechoic and calcified. Chronic thrombosis narrows the vessel diameter and results in the loss of a spectral curve. In cases of acute or subacute thrombosis, subcutaneous edema may also be detected (Figs. 10, 11) [29].
Steal Syndrome
Dialysis access-related steal syndrome (DASS) is an uncommon but recognized complication that most commonly affects smokers, patients with diabetes, and elderly individuals (aged 80 years and older). DASS more frequently occurs in patients with AVGs than in those with AVFs [31]. Among patients with AVFs, steal syndrome is more common in those whose access is supplied by the brachial artery [32]. Symptomatic ischemia in the distal upper extremity is seen in 10% to 25% of patients with brachiocephalic and brachiobasilic vascular access, while only 1% to 2% of patients with radiocephalic AVFs experience symptomatic ischemia [33]. Typically, patients who experience this complication begin showing symptoms during their dialysis session.
DASS is a result of arterial insufficiency that occurs distal to the AVF. This condition implies that the bulk of the arterial blood supply is directed into the anastomosis instead of the distal artery. This diversion can lead to hand ischemia, hypoxia, and necrosis [1]. In parallel, an increase in flow occurs within the fistula along with bidirectional flow in the distal artery. These phenomena are clearly depicted on US images [27,34,35].
Treatment of this condition presents challenges, including a high risk of finger and forearm amputation. The preferred method for managing hand ischemia while preserving the AVF is the distal revascularization-interval ligation procedure [31]. However, in severe instances, it may be necessary to completely abandon the access through surgical ligation.
Aneurysms, Pseudoaneurysms, and Hematomas
An important category of complications related to upper extremity vascular access involves vein wall injuries that result in aneurysms, pseudoaneurysms, and hematomas [29]. An aneurysm is a condition where a portion of the artery wall weakens, affecting all three layers of the vessel wall and causing abnormal dilation. A pseudoaneurysm is essentially a contained vessel leak that occurs due to iatrogenic trauma in situations involving repetitive access punctures [36]. Unlike hematomas, pseudoaneurysms maintain a connection with the vessel lumen [29].
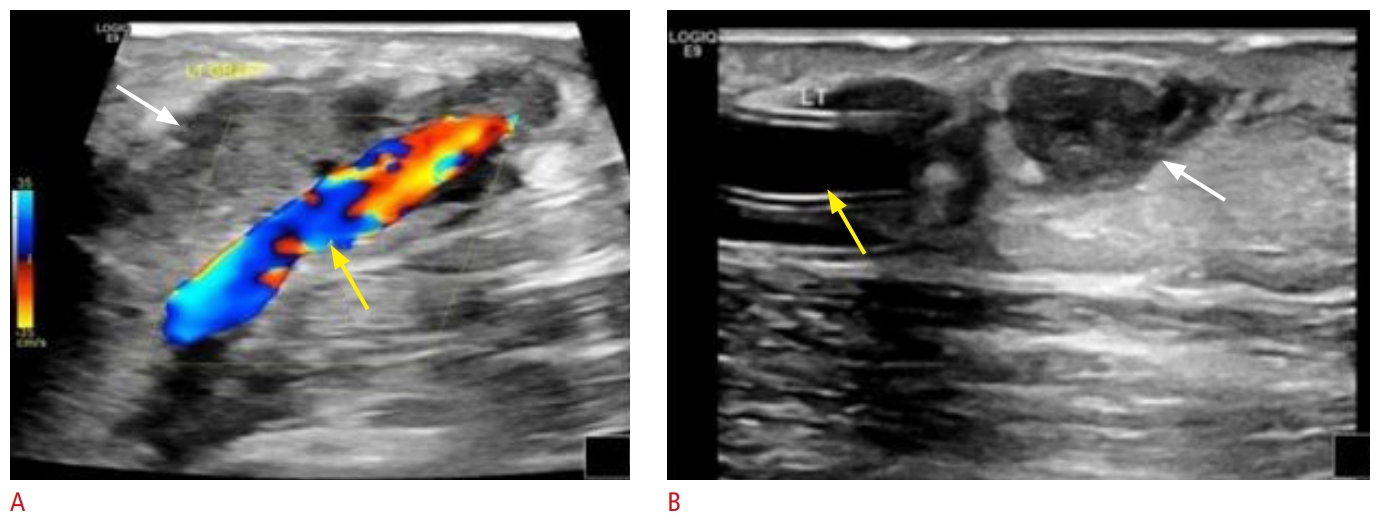
Color Doppler US is essential for the evaluation of a focal mass at the upper extremity vascular access site. This modality enables the differentiation of aneurysms, pseudoaneurysms, and hematomas from an acutely thrombosed bulky vascular access, also known as a pseudomass. Pseudoaneurysms often manifest as a pulsatile mass. When examined with color Doppler US, they exhibit the distinctive "yin-yang sign" or swirling flow pattern, as well as bidirectional flow that has been characterized as displaying a "to-and-fro pattern" at the neck of the pseudoaneurysm [1,29]. Hematomas present as a heterogeneous fluid collection, primarily extending into the adjacent musculature and subcutaneous tissues (Fig. 12) [29]. In contrast, aneurysms appear as a saccular dilation of all layers of the affected vasculature. The complexity of endovascular and surgical treatment options is beyond the scope of this article [29,37].
Infection
Although it has been reported that the infection rate of AVFs is one-tenth the infection rate of AVGs [38], infections still represent up to 20% of all complications associated with AVFs [25,38]. These infections can vary in severity, from perivascular cellulitis and edema to more serious conditions such as abscesses that necessitate percutaneous drainage (Fig. 13) [38]. Symptoms may include redness or pain at the site of vascular access, along with systemic signs such as fever and chills [29]. Infection diagnosis is typically clinical, and US plays a limited role. It is primarily used to verify graft patency and functionality, as well as to identify any drainable abscesses [29].
Ischemic Neuropathy
Ischemic polyneuropathy is a rare complication of AVF that typically develops rapidly within the first few hours following AVF creation [29]. This condition predominantly affects female and diabetic patients with preexisting neuropathy [29]. The clinical symptoms include weakness in the distal muscle groups, intense pain, and paresthesia. The affected hand is usually warm, and a palpable radial pulse or a detectable Doppler US signal is often present [39]. The etiology of this complication is believed to be acute limb ischemia, which occurs when arterial blood is diverted away from the distal extremity after the creation of an AVF, leading to multiple axonal loss mononeuropathies in these patients [39]. US does not play a significant role in diagnosing ischemic neuropathy, which is primarily determined based on clinical parameters.
Exacerbation of Congestive Heart Failure
AVFs increase cardiac output, potentially leading to detrimental effects on cardiac function, especially in the context of preexisting heart disease [29]. Research has shown that the creation of AVFs in patients with ESRD can lead to increased instances of left ventricular hypertrophy, pulmonary hypertension, right ventricular dysfunction, coronary artery disease, and valvular heart disease [40,41].
Stenosis
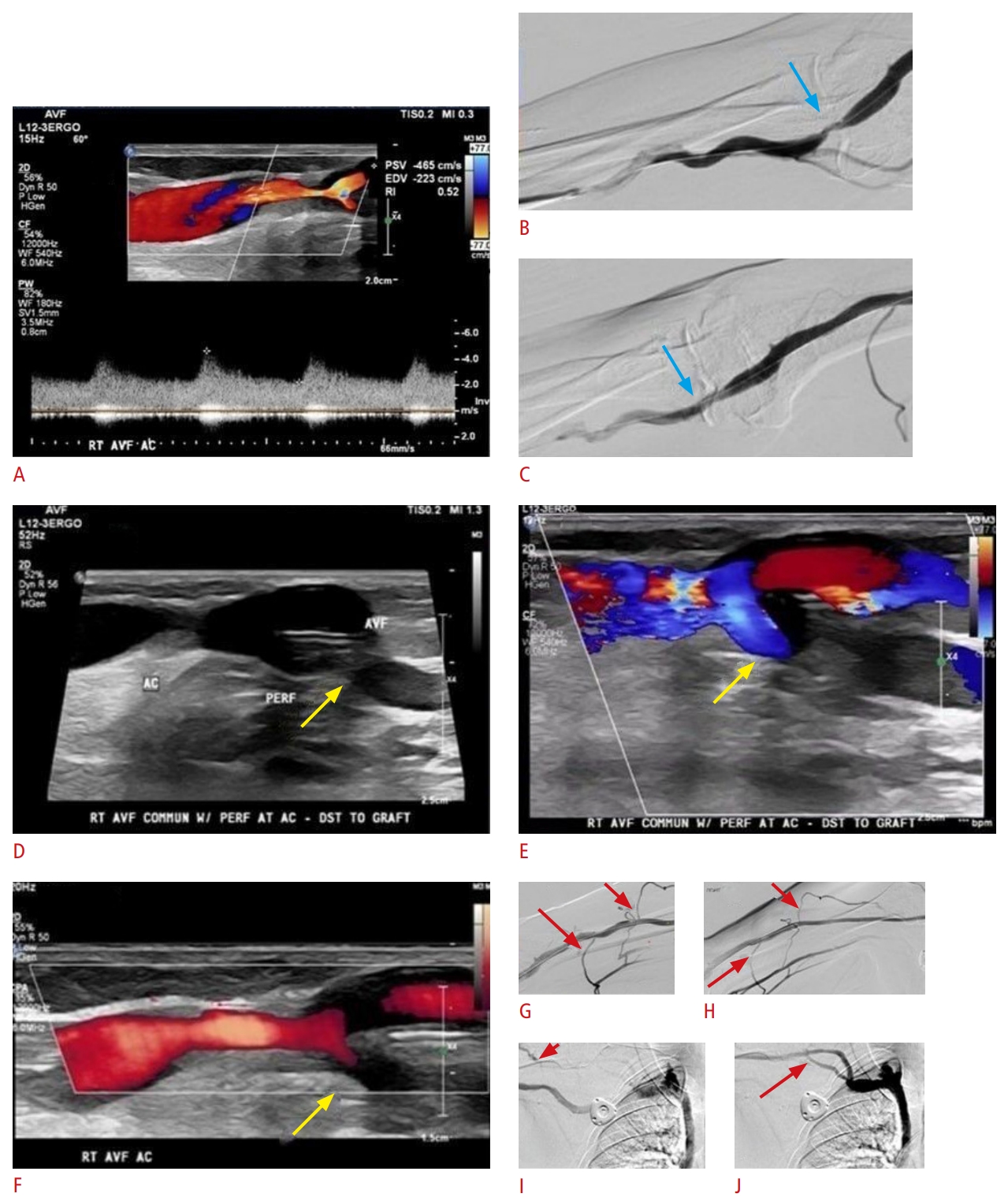
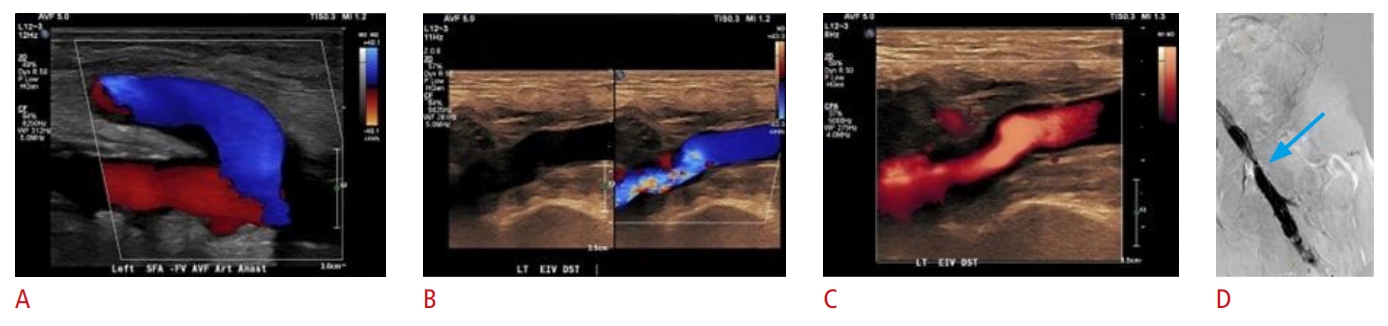
Stenotic disease in AVFs and AVGs is characterized by the narrowing of the vessel lumen due to neointimal hyperplasia or a partially obstructive thrombus [29]. This narrowing results in elevated venous pressures and poor flow rates during dialysis (Fig. 14) [29]. The risk of thrombosis generally increases with the degree of stenosis. In AVFs, stenosis most frequently occurs in the juxta-anastomotic segment (80%). This type of stenosis impacts the initial 2 cm of the draining vein near the arteriovenous anastomosis, which can ultimately lead to early fistula failure (Figs. 15, 16) [29]. In the case of AVGs, stenoses predominantly occur at the venous anastomoses and occasionally at the draining vein, central vein, feeding artery, or within the graft lumen [1]. Signs of an underlying stenosis may include AVF/AVG dysfunction, difficulties with cannulation zone puncture, pain at the fistula site, and elevated venous pressures.
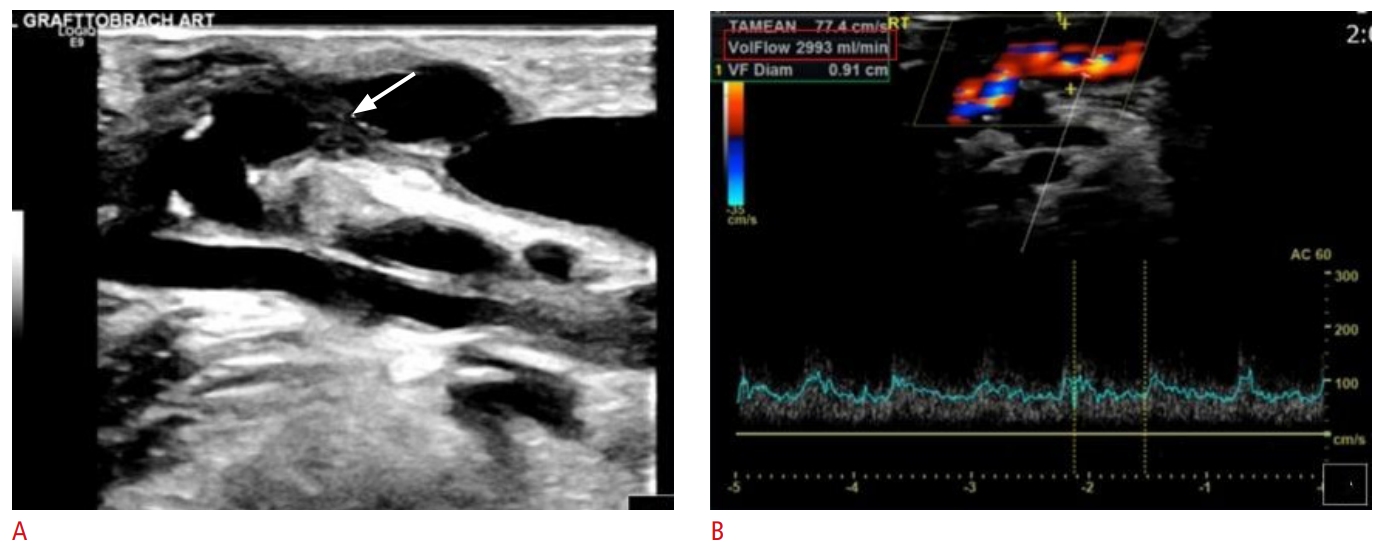
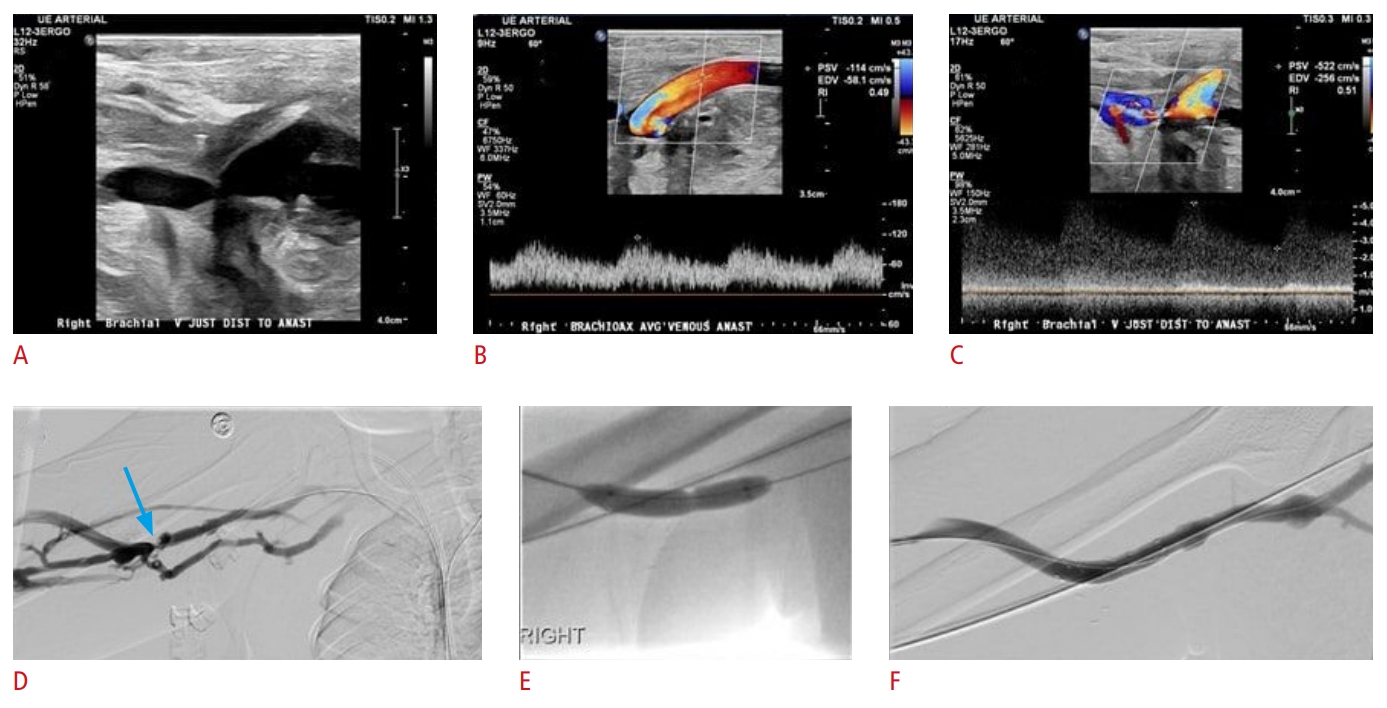
Color and spectral Doppler techniques are the most accurate noninvasive methods for diagnosing stenoses, as they can identify lumen narrowing and facilitate measurements of PSV. US criteria for stenosis encompass morphological and hemodynamic factors, as well as changes in velocity. Morphologically, arterial stenosis is deemed critical based on a 60% to 75% vessel narrowing, while venous stenosis is considered critical with a 50% reduction in vessel diameter [29]. Hemodynamically, aliasing and color turbulent (variant) flow on color Doppler US suggest underlying stenotic disease. On spectral Doppler US, PSV values exceeding 200 to 250 cm/s at the tributary artery or over 300 to 400 cm/s in the outflow vein are direct indicators of stenosis [29]. Stenosis over 50% is characterized by a 3:1 PSV ratio measured at the stenosis and 2 cm cephalad, as well as a doubling of PSV in the draining vein (Figs. 17, 18) [1,29]. Published guidelines (Table 2) have established basic criteria for the presence of significant stenosis in upper extremity vascular access, which include a narrowing of the vascular lumen over 50% and a PSV ratio (the ratio between PSV in the stenotic and pre-stenotic area) over 2. Additionally, at least one of the following criteria must be present: blood flow less than 500 mL/min in AVFs or less than 600 mL/min in AVGs, a blood flow reduction of more than 25% in cases of blood flow less than 1,000 mL/min, and/or a residual patent diameter of the examined vessel less than 2 mm [42]. For AVGs, when no additional criteria are present, the detected stenosis is classified as borderline. In these instances, a repeat scan may be considered after 6 to 8 weeks [43]. A narrow graft diameter toward the arterial anastomosis may be associated with expected and unremarkable postoperative changes, and this may have the benefit of reducing the risk of steal phenomena leading to hand ischemia [7]. The treatment of stenotic disease is beyond the scope of this article and may involve angioplasty, including the use of drug-coated balloons, stent-graft placement, or surgical revision [29,36].
Novel Developments of Multiparametric US
The term "multiparametric US" was introduced to describe the diverse aspects and complementary tools of US [44]. This umbrella term includes conventional anatomic techniques such as grayscale B-mode; the spectrum of Doppler techniques including color, power, and spectral Doppler; and recent advances such as non-Doppler flow visualization techniques, contrast-enhanced US, and elastography. The application of these various techniques has been demonstrated beneficial across a range of organs and clinical situations, including carotid atherosclerotic disease [45-47]. Table 3 outlines the future potential of multiparametric US in the context of vascular access assessment. Advanced techniques may help overcome obstacles and serve as a problem-solving tool in complex cases. Fig. 19 provides a representative example of the use of elastography in a case of AVF thrombosis.
Conclusion
A functional venous access, in the form of an AVF or AVG, enhances the quality of life among patients with ESRD by facilitating safe and effective hemodialysis. However, upper extremity vascular accesses require endovascular maintenance due to the risk of failure and potential complications. US plays a pivotal role not only in preoperative planning and mapping of the upper extremity vasculature, but also in monitoring the function and patency of AVFs and AVGs. This allows clinicians to detect complications and impending failure early. These US findings substantially contribute to the management of the ESRD patient population. Utilizing various blood-flow visualization techniques, US is the noninvasive imaging modality of choice for evaluating upper extremity vascular accesses.




 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI



