

 Print
Print facebook
facebook twitter
twitter Linkedin
Linkedin google+
google+

Introduction
The first trimester of pregnancy consists of the first 12-13 weeks, calculated as beginning on the first date of the last menstrual period (LMP). During the first trimester, transvaginal ultrasonography (TVUS) is the imaging modality of choice for both diagnosis and imaging follow-up. The advantages of ultrasound imaging include its widespread availability, relatively low cost, and the acquisition of real-time, high-resolution images. The initial diagnosis of pregnancy is usually made by identifying the presence of serum beta-human chorionic gonadotropin (β-hCG). Ultrasound is then utilized during the first and second trimesters to establish the gestational age of the pregnancy and eventually to evaluate fetal anatomy. In the first trimester, pelvic ultrasound is employed to establish the presence or absence of an intrauterine gestational sac and to evaluate the viability of the pregnancy. In addition, it can be used to evaluate ectopic pregnancy and other pregnancy-related complications. Practice parameters for the performance and recording of obstetric ultrasound images have been described by the American Institute of Ultrasound in Medicine [1].
Timeline of First-Trimester Sonographic Findings
Gestational Sac
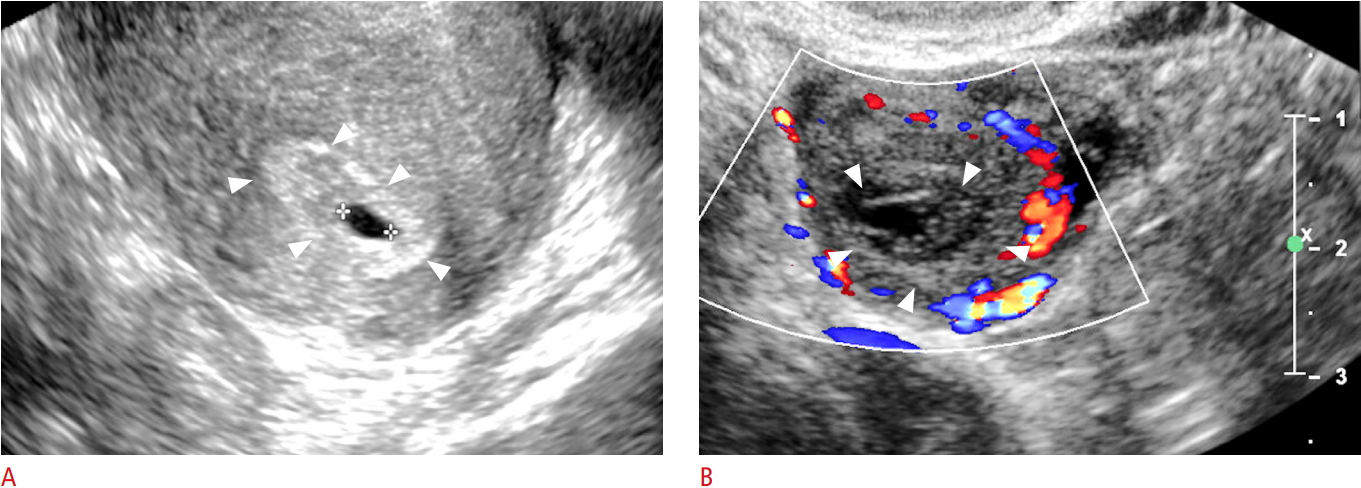
Conventionally, gestational age is initially calculated from the first day of the LMP. Ovulation typically occurs mid-cycle, at about day 14 of the menstrual cycle, at which point fertilization (conception) is most likely to occur. Thus, by the time of the first missed menstrual period, fertilization and implantation of the fertilized ovum have occurred. During the first 3 weeks following conception, the developing gestational sac is below the limit of detection by TVUS [2]. The growth rate of the gestational sac is approximately 1.1 mm/day and the gestational sac first becomes apparent on TVUS at approximately 4.5-5 weeks of gestational age, appearing as a round anechoic structure located eccentrically within the echogenic decidua (Table 1, Fig. 1A, B) [3].
Double Decidual Sac Sign
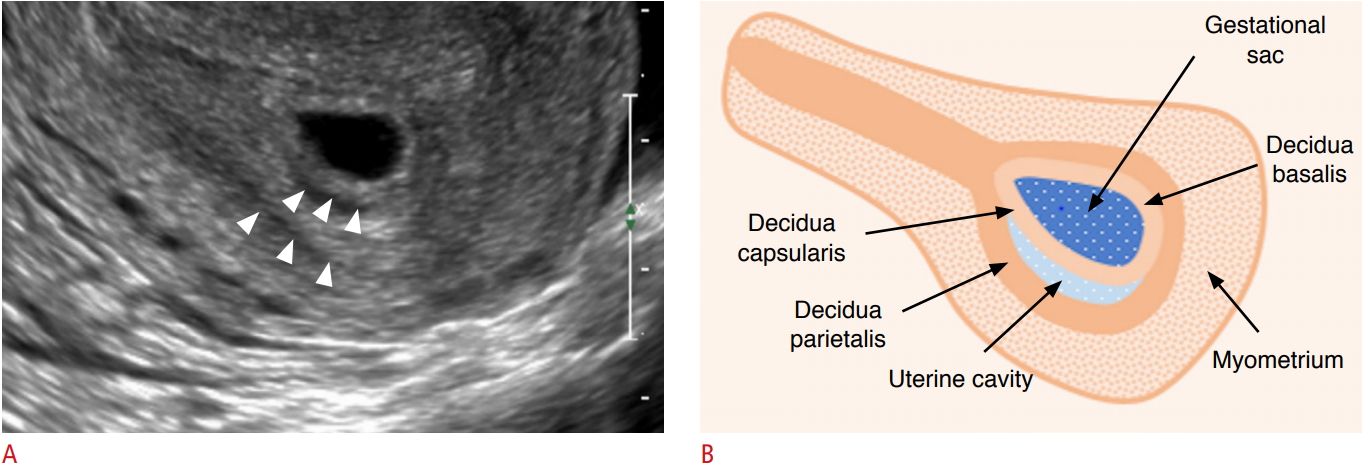
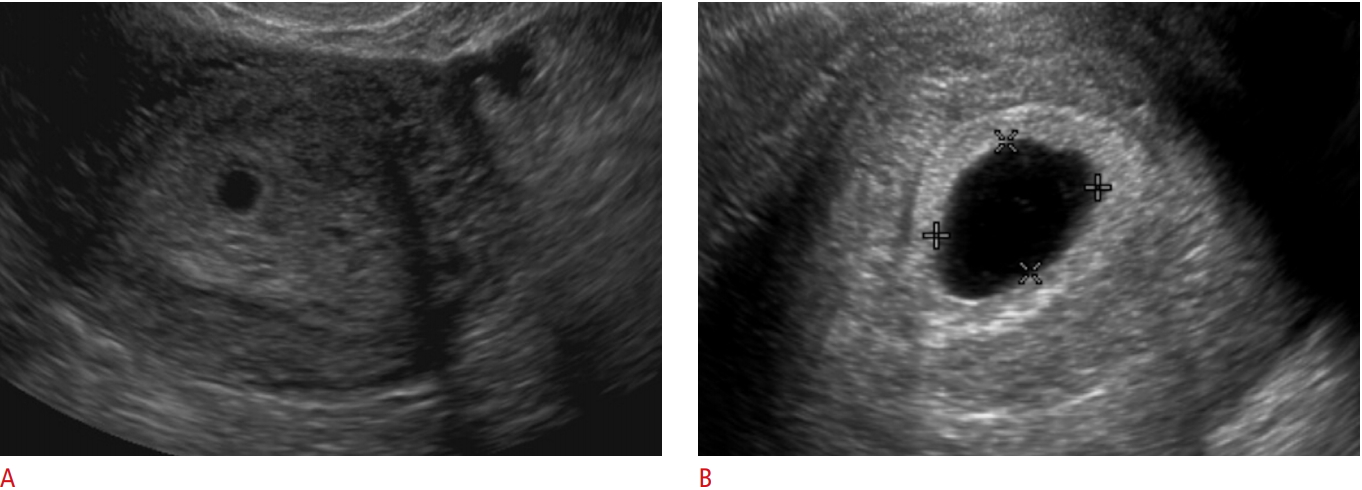
Subsequent to the appearance of the gestation sac, two concentric echogenic rings encircling the central anechoic collection develop: the outer ring represents the decidua parietalis, while the inner ring represents the decidua capsularis and chorion (Fig. 2A, B). This is known as the double decidual sac sign (DDS), which is a definitive sign of an intrauterine pregnancy (IUP). While the presence of the DDS sign confirms an IUP, its absence does not exclude an IUP [4]. Furthermore, the DDS sign can be difficult to demonstrate sonographically. For this reason, the possibility of a gestational sac should be considered for any round or ovoid fluid collection within the endometrium (Fig. 3A, B) [4]. Gestational sac size is measured in 3 dimensions and the mean sac diameter (MSD) is used to help estimate the early gestational age.
Yolk Sac
At around 5.5 weeks of gestation, the developing yolk sac becomes visible. Initially appearing as two echogenic parallel lines at the periphery of the gestational sac, the yolk sac eventually acquires its typical round appearance by the end of 5.5 weeks [2].
Embryo
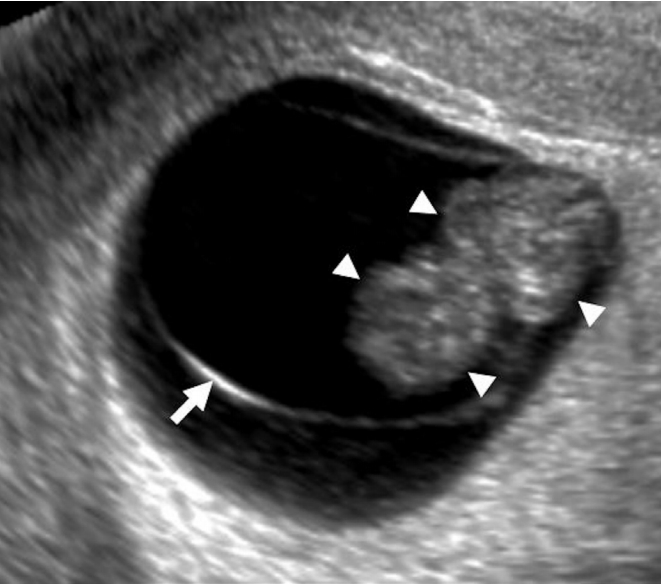
The embryo (sometimes referred to as the fetal pole early on) becomes apparent at 6 weeks of gestation as a relatively featureless echogenic linear or oval structure adjacent to the yolk sac, initially measuring 1-2 mm in length. At this point, the MSD is approximately 10 mm. The crown-rump length (CRL) is the measurement between the cranial and caudal ends of the embryo and is the most accurate measure of the gestational age in the first trimester. The CRL gradually increases, measuring 10 mm at 7.0 weeks. The lack of a visible embryo on TVUS once the MSD reaches at least 25 mm is diagnostic of pregnancy failure (Fig. 4) [2,5]. While the fetal pole begins as a featureless structure, some fetal anatomic structures become visible as the first-trimester progresses. The spine appears at 7-8 weeks, and the hindbrain (rhombencephalon) is evident at 8-10 weeks [6].
Amniotic Membrane
The amniotic membrane becomes visible around 7 weeks, and the CRL closely corresponds to the amniotic sac diameter between 6.5 and 10 weeks of gestation (Fig. 5) [7]. After fetal urine production commences at about 10 weeks, there is a disproportionate enlargement of the amniotic sac relative to the chorionic cavity. The amnion and chorion fuse after the first trimester at 14-16 weeks [8].
Cardiac Activity
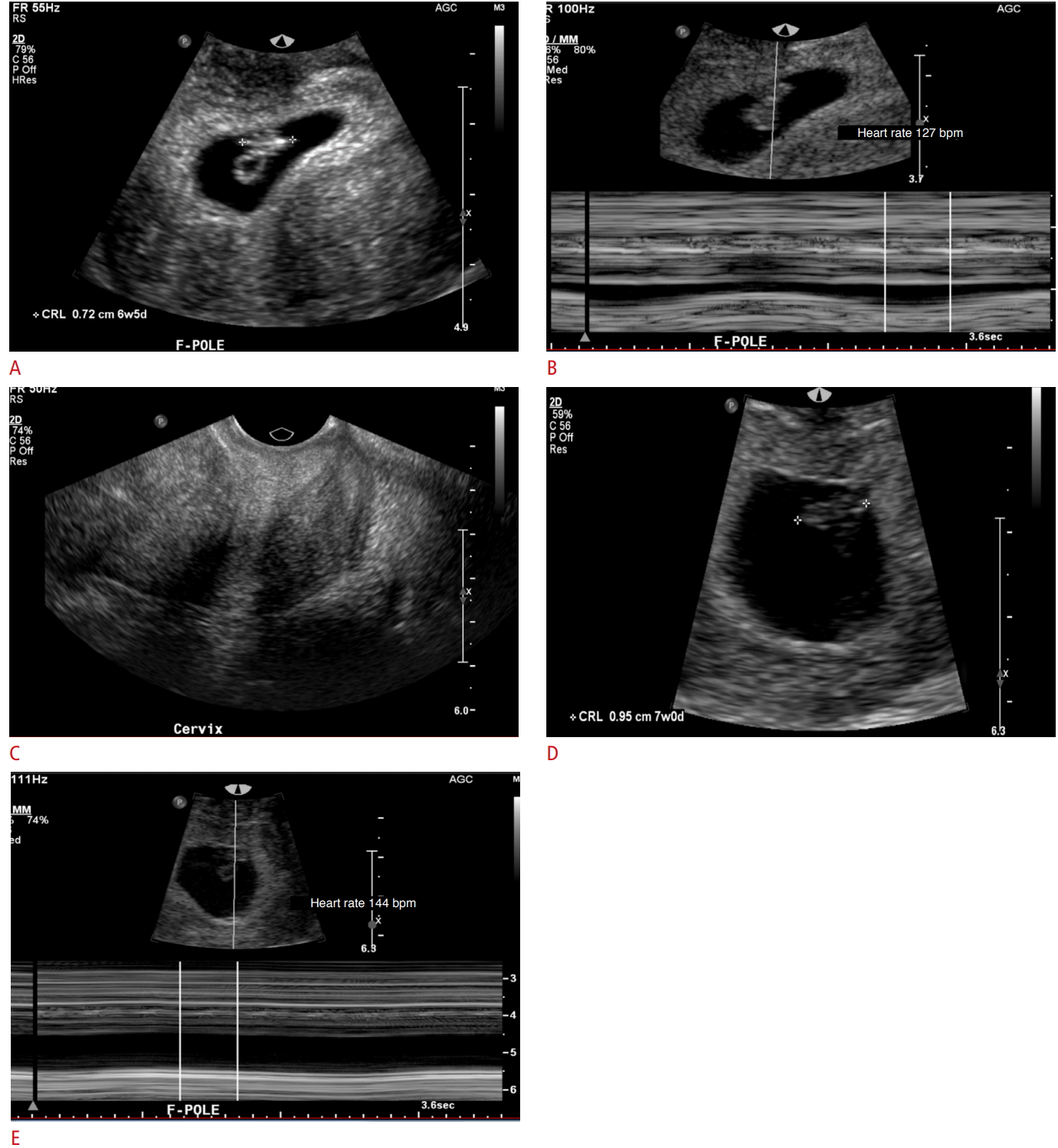
Cardiac activity is seen as early as the sixth week of gestation, when the embryo is 1-2 mm in size. The current guidelines of the Society of Radiologists in Ultrasound (SRU) establish a CRL cutoff of 7 mm, above which one should definitively visualize fetal cardiac activity. The absence of a detectable heartbeat once the embryo measures greater than 7 mm in length is diagnostic of pregnancy failure (Fig. 6A, B) [7]. The fetal heart rate gradually increases with gestational age from approximately 110 beats per minute (bpm) at 6.2 weeks to approximately 159 bpm at 7.6-8.0 weeks (Fig. 7A-E) [9]. Slow embryonic heart rates are associated with a worse shortterm prognosis, with fetal heart rates less than 100 bpm before 6.3 weeks or below 120 bpm at 6.3-7.0 weeks linked to an increased rate of embryonic demise [9,10]. The overall prognosis improves with increasing heart rate [10].
First-Trimester Abnormalities
First-trimester TVUS is routinely performed in patients presenting with pelvic/abdominal pain or vaginal bleeding. Once pregnancy is established with urine or serum β-hCG tests, the utility of TVUS for evaluation of these patients is multifactorial: (1) to determine the presence and multiplicity of an IUP, (2) to determine the viability of an IUP, (3) to determine the stage of spontaneous abortion in the case of a nonviable pregnancy, and (4) to identify probable reasons why an IUP is not identified on TVUS.
Confirming an IUP
The detection of an eccentrically-located, anechoic collection in the endometrium of a patient with elevated serum β-hCG levels represents an IUP in 99.5% of cases [4]. The presence of two or more gestational sacs surrounded by thick echogenic chorion, or sonographic features of the inter-twin membrane and "twin-peak" sign, confirm a multiple-gestation pregnancy [11].
Evaluating Viability
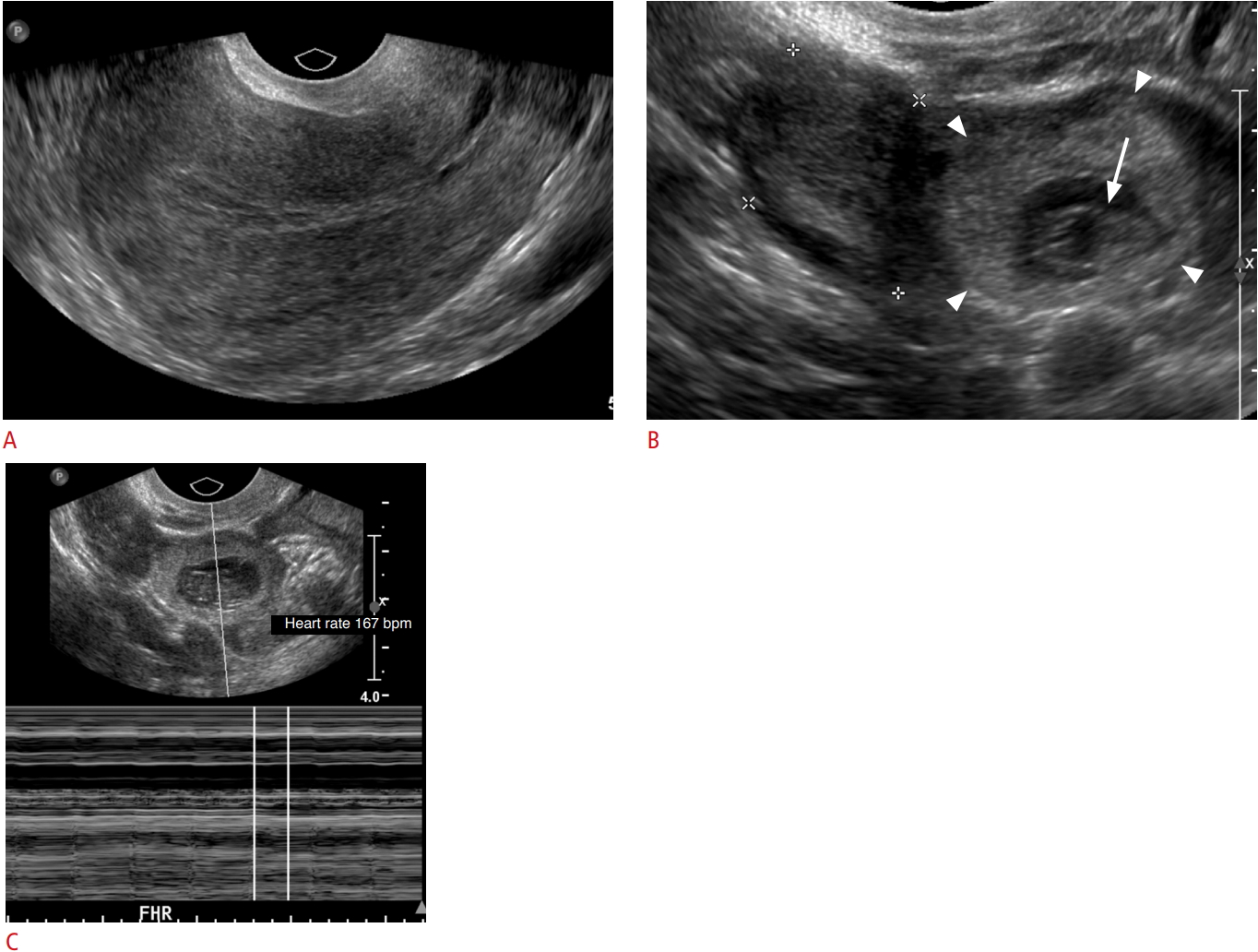
Once an IUP is identified, the viability and presence or absence of abnormal features must be evaluated. The timeline of visualization of the gestational sac, yolk sac, and embryo at 5, 5.5, and 6 weeks, respectively, are accurate and consistent [5]. Deviations from the normal chronological appearance of these structures are highly suspicious for pregnancy failure. The SRU has presented specific guidelines for diagnosing pregnancy failure based on certain characteristics: namely, (1) the CRL measurement by which an embryonic heart rate must be identified (7 mm), (2) the MSD by which an embryo should be identified (25 mm), and (3) the absence of an embryo in two consecutive ultrasound exams separated by a fixed time interval. In addition, other findings including the empty amnion sign, a yolk sac greater than 7 mm, and a disproportionately small gestational sac are highly suspicious for pregnancy failure (Fig. 8). Through these guidelines, the SRU aims to achieve 100% specificity for defining pregnancy failure and to sustain a primum non nocere approach given the calamitous outcome of a potentially normal pregnancy following treatment for an incorrectly diagnosed pregnancy failure (Table 2) [4,5].
Subchorionic Hematoma
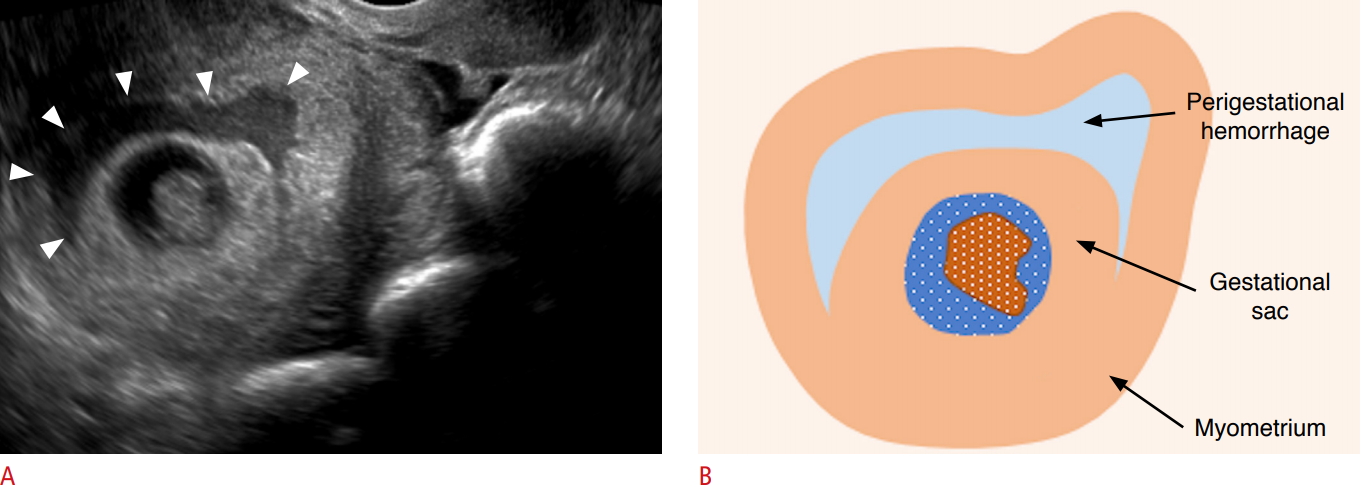
Subchorionic hematoma (SCH) is a relatively common finding in the first trimester and has been reported to occur in 18%-22% of IUPs in patients presenting with vaginal bleeding [12,13]. On TVUS, SCH appears as a crescent-shaped, heterogeneous avascular collection between the gestational sac and decidua basalis (Fig. 9A, B). Larger subchorionic hematomas are associated with an increased risk of pregnancy loss, especially if the hematoma is greater than twothirds of the chorionic circumference [13,14].
Spontaneous Abortion
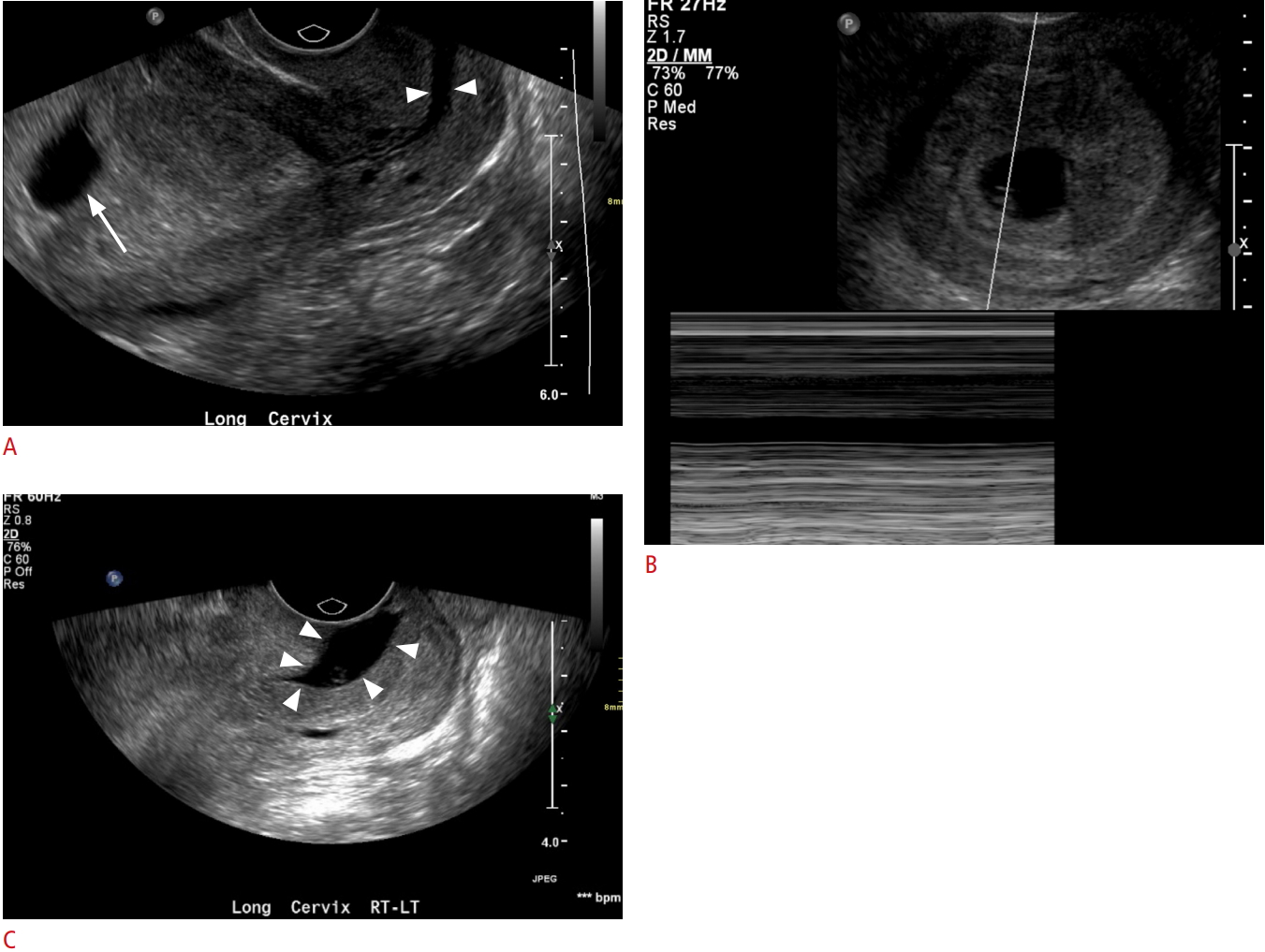
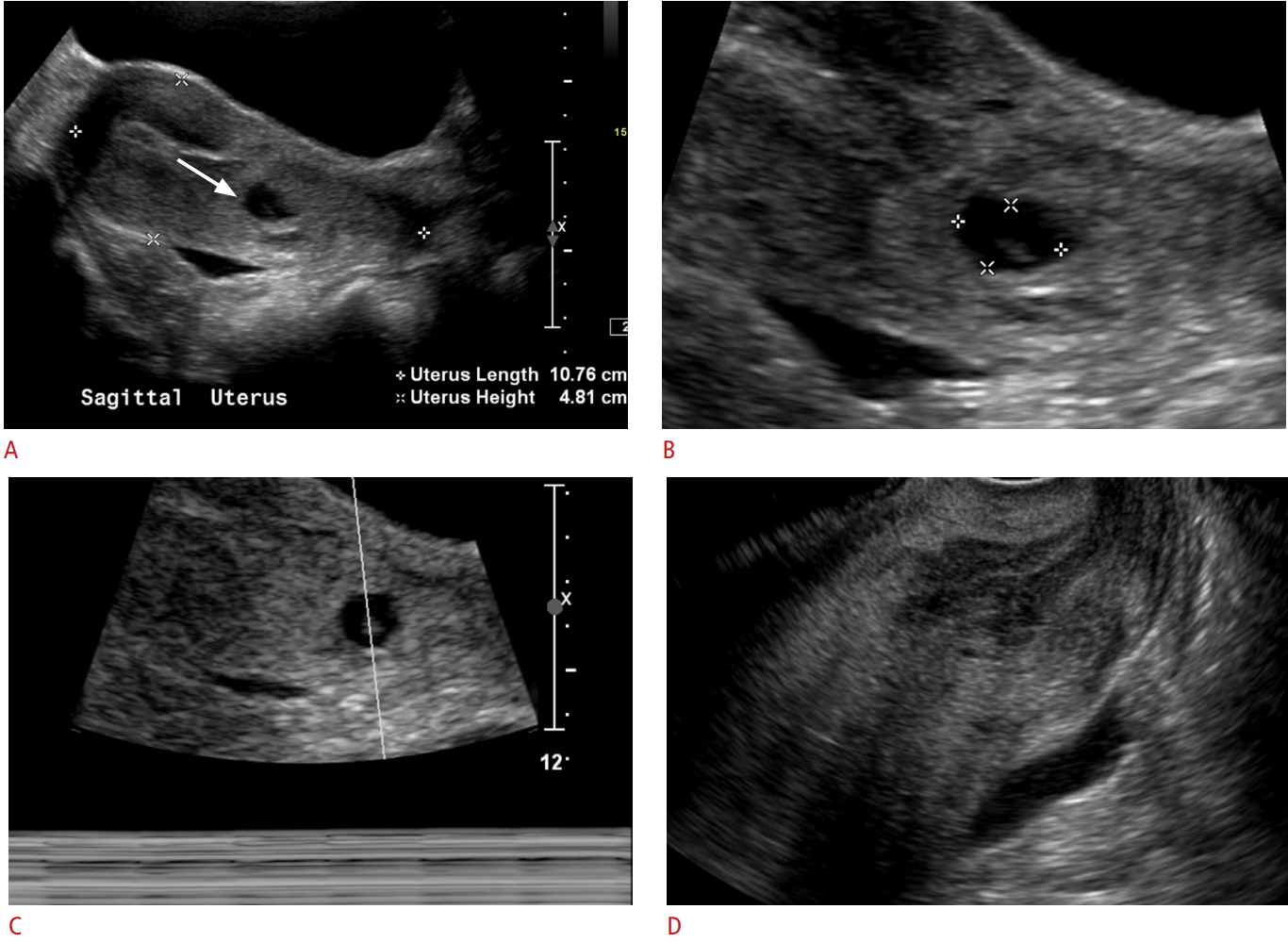
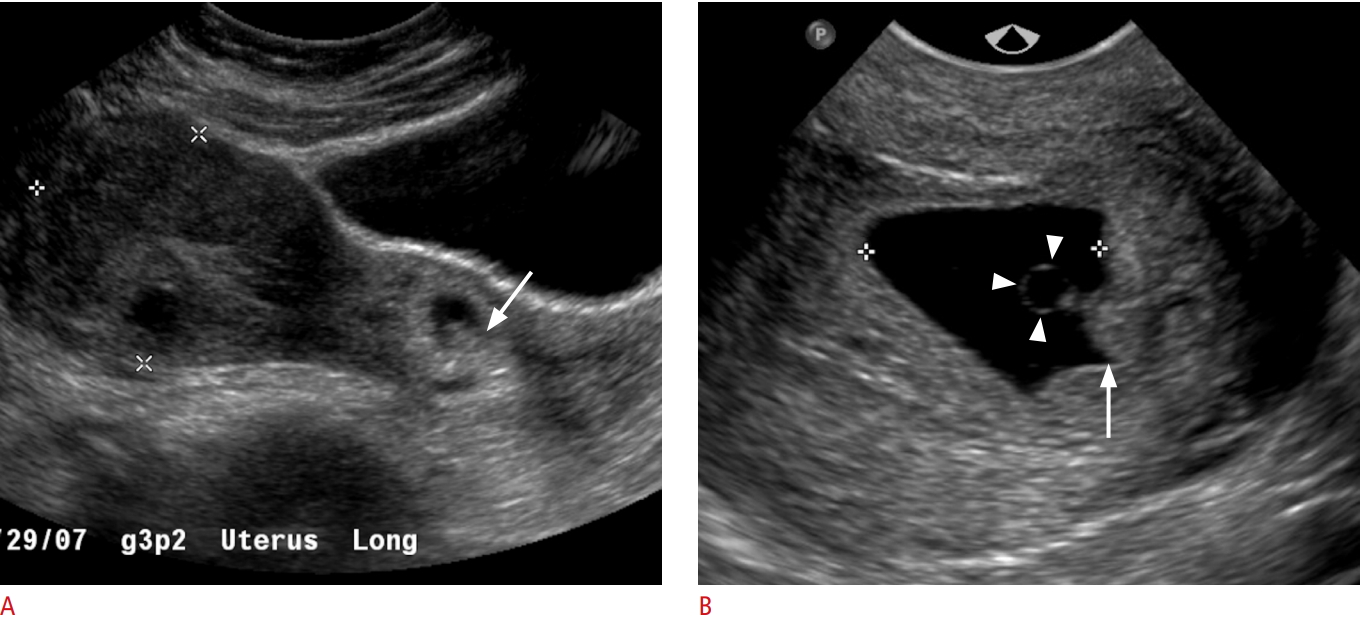
Spontaneous abortion or miscarriage is clinically defined as the loss of a pregnancy before the 20th week of gestation or the expulsion of a fetus weighing less than 500 g [15,16]. There are various stages of spontaneous abortion. A threatened abortion refers to a clinical scenario in which a patient presents with vaginal spotting/bleeding and cramping/contractions with a closed cervical os. The pregnancy itself may appear normal or may demonstrate abnormal features. Poor prognostic indicators include abnormal morphology (e.g., a small or irregular gestational sac), fetal bradycardia, or a large SCH [9,12]. An inevitable abortion involves a similar clinical situation with vaginal bleeding and abdominal cramping, but with an open cervical os on TVUS (Fig. 10A-C). The products of conception may be normally or abnormally positioned within the uterus or may protrude into the cervix. An incomplete abortion is the term used when the retained products of conception remain within the uterus after passage of the pregnancy. This often appears as a heterogeneous collection or mass within the uterus. While it may be avascular, the presence of blood flow enables the diagnosis of retained products. A completed abortion is the cessation of vaginal bleeding following the passage of the pregnancy without retained products of conception (Fig. 11A-D). Lastly, a missed abortion is a nonviable pregnancy with a closed cervix and no clinical symptoms of miscarriage [17].
Pregnancy of Unknown Location and Ectopic Pregnancy
In a substantial number of patients evaluated in the emergency department during very early pregnancy, the location of the gestational sac is inconclusive. The significance of a nonvisualized gestational sac on TVUS in a patient with a positive pregnancy test could reflect one of three scenarios: (1) less than 5 weeks of gestation, (2) ectopic pregnancy, or (3) a completed abortion [18].
It is incumbent for the technologist/radiologist to carefully scrutinize the adnexa and other spaces in the pelvis for any masses, collections, or obvious products of conception in order to rule out an ectopic pregnancy. As the prevalence of ectopic pregnancy is 1.4% and it accounts for 25% of all maternal deaths, practitioners should have a high degree of suspicion for this diagnosis. Although the vast majority of ectopic pregnancies occur in the fallopian tubes, implantation of pregnancies at other sites can also take place, including the cervix, cesarean scars, uterine cornua, and other nongynecological sites in the abdomen and pelvis (Figs. 12-14) [2]. In cases in which no IUP is identified and there is no sonographic evidence of an ectopic pregnancy, serial monitoring of β-hCG levels and short-term repeat TVUS are generally recommended for follow-up.
Gestational Trophoblastic Disease
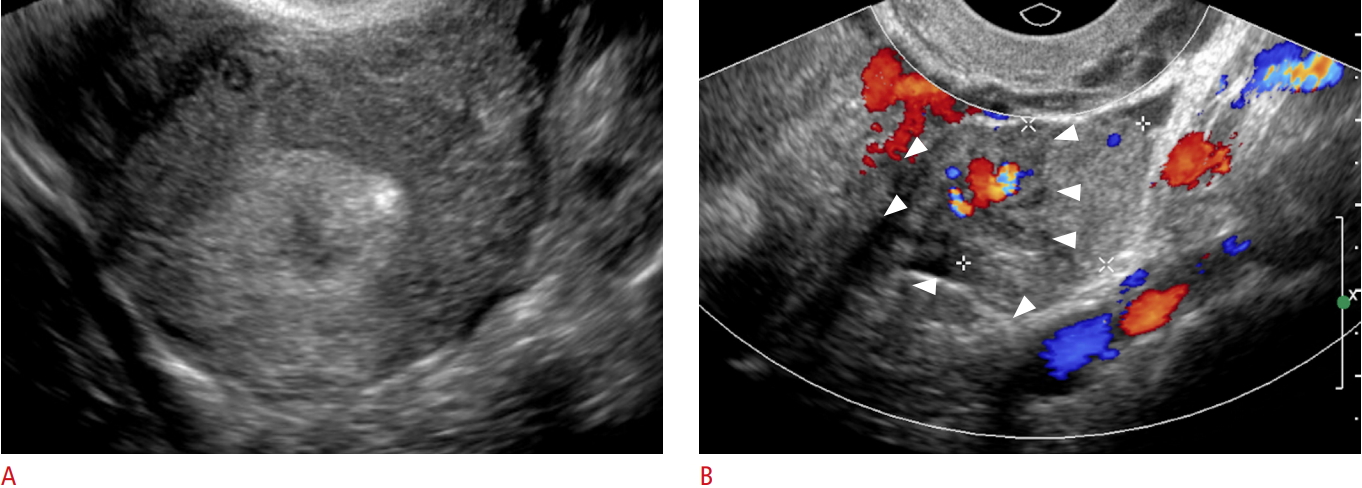
Gestational trophoblastic disease is a broad term which encompasses both benign entities, such as partial and complete mole, gestational trophoblastic neoplasia (GTN), and malignant diagnoses, such as invasive mole, choriocarcinoma, and epithelioid and placental site trophoblastic tumors. As a result of dispermic fertilization of an ovum, pregnant patients will often present with vaginal bleeding. On TVUS in the first trimester, the endometrial cavity will contain an echogenic solid mass, usually with numerous cystic spaces, which are the hydropic villi and trophoblastic hyperplasia (Fig. 15). Careful scrutiny of the mass is important to distinguish between complete mole (no fetal parts), partial mole (some fetal parts), and GTN (myometrial invasion) [19].
Conclusion
The diagnostic possibilities for pregnant patients presenting with pain and bleeding are broad. TVUS is paramount in its utility as a diagnostic tool for these patients. When used in combination with clinical information and serum β-hCG levels, it can provide diagnostic and prognostic information to clinicians regarding pregnancy confirmation and viability, as well as rapid information regarding life-threatening conditions such as ectopic pregnancy.




 Download Citation
Download Citation PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC



